

Clinical risk factors for increased respiratory drive in intubated hypoxemic patients
- PMID: 37041553
- PMCID: PMC10088111
- DOI: 10.1186/s13054-023-04402-z
Clinical risk factors for increased respiratory drive in intubated hypoxemic patients
Abstract
Background: There is very limited evidence identifying factors that increase respiratory drive in hypoxemic intubated patients. Most physiological determinants of respiratory drive cannot be directly assessed at the bedside (e.g., neural inputs from chemo- or mechano-receptors), but clinical risk factors commonly measured in intubated patients could be correlated with increased drive. We aimed to identify clinical risk factors independently associated with increased respiratory drive in intubated hypoxemic patients.
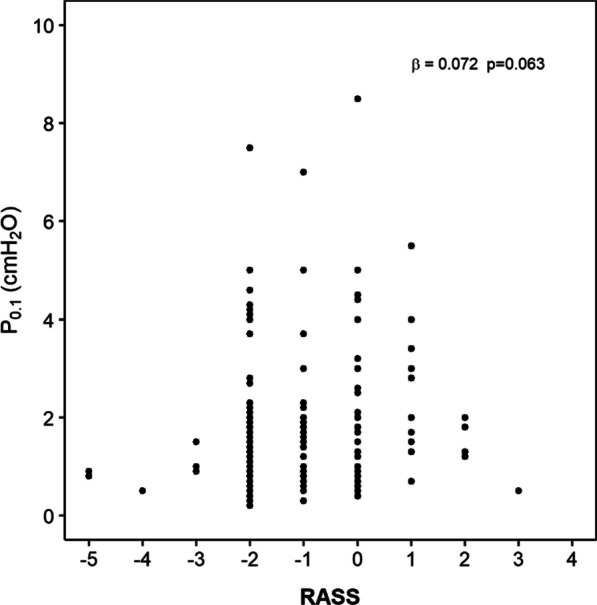
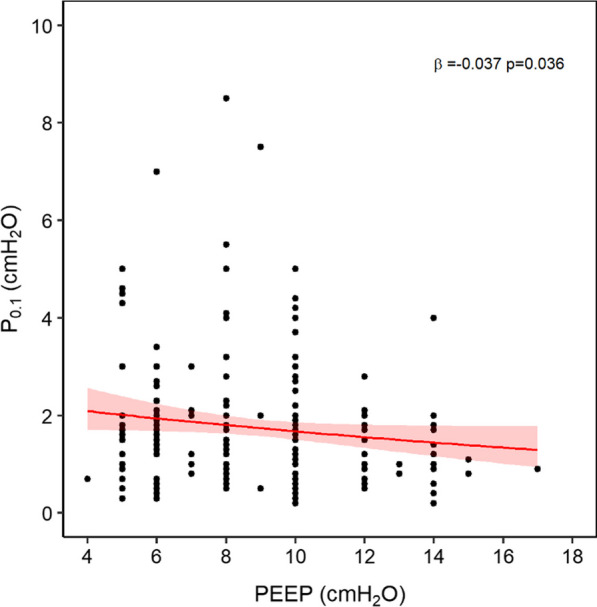
Methods: We analyzed the physiological dataset from a multicenter trial on intubated hypoxemic patients on pressure support (PS). Patients with simultaneous assessment of the inspiratory drop in airway pressure at 0.1-s during an occlusion (P0.1) and risk factors for increased respiratory drive on day 1 were included. We evaluated the independent correlation of the following clinical risk factors for increased drive with P0.1: severity of lung injury (unilateral vs. bilateral pulmonary infiltrates, PaO2/FiO2, ventilatory ratio); arterial blood gases (PaO2, PaCO2 and pHa); sedation (RASS score and drug type); SOFA score; arterial lactate; ventilation settings (PEEP, level of PS, addition of sigh breaths).
Results: Two-hundred seventeen patients were included. Clinical risk factors independently correlated with higher P0.1 were bilateral infiltrates (increase ratio [IR] 1.233, 95%CI 1.047-1.451, p = 0.012); lower PaO2/FiO2 (IR 0.998, 95%CI 0.997-0.999, p = 0.004); higher ventilatory ratio (IR 1.538, 95%CI 1.267-1.867, p < 0.001); lower pHa (IR 0.104, 95%CI 0.024-0.464, p = 0.003). Higher PEEP was correlated with lower P0.1 (IR 0.951, 95%CI 0.921-0.982, p = 0.002), while sedation depth and drugs were not associated with P0.1.
Conclusions: Independent clinical risk factors for higher respiratory drive in intubated hypoxemic patients include the extent of lung edema and of ventilation-perfusion mismatch, lower pHa, and lower PEEP, while sedation strategy does not affect drive. These data underline the multifactorial nature of increased respiratory drive.
Keywords: Acute respiratory failure; Positive end-expiratory pressure; Respiratory drive; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
PN received personal fees for lectures from Fisher and Paykel, Mindray, Hamilton, outside of the submitted work. TM received personal fees for lectures from Drager, Mindray and Fisher and Paykel, outside of the submitted work. All other authors declare that they have no competing interests.
Figures


References
-
- Bruce EN, Cherniack NS. Central chemoreceptors. J Appl Physiol. 1985;1987(62):389–402. - PubMed
