Interrater Reliability of Functional Lumen Imaging Probe Panometry and High-Resolution Manometry for the Assessment of Esophageal Motility Disorders
- PMID: 37042784
- PMCID: PMC10523887
- DOI: 10.14309/ajg.0000000000002285
Interrater Reliability of Functional Lumen Imaging Probe Panometry and High-Resolution Manometry for the Assessment of Esophageal Motility Disorders
Abstract
Introduction: High-resolution manometry (HRM) and functional lumen imaging probe (FLIP) are primary and/or complementary diagnostic tools for the evaluation of esophageal motility. We aimed to assess the interrater agreement and accuracy of HRM and FLIP interpretations.
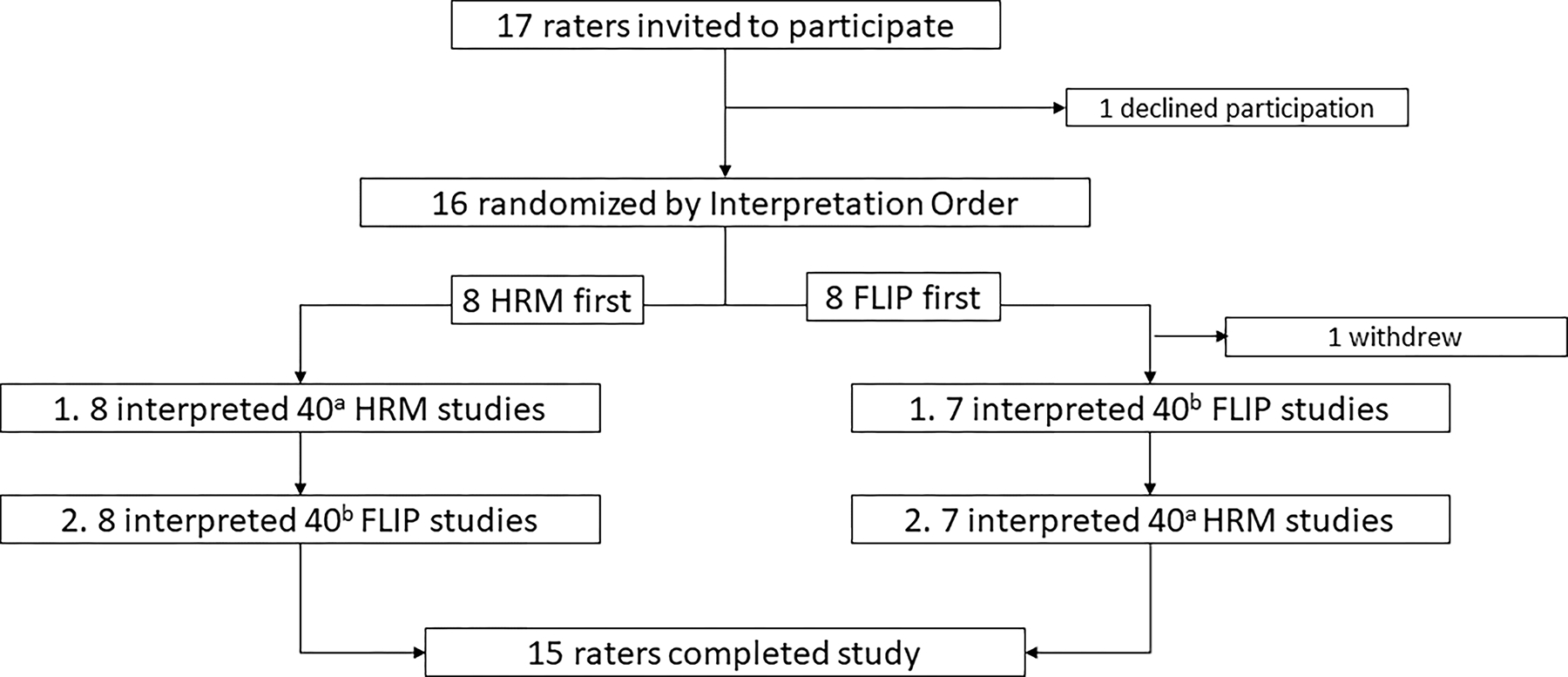
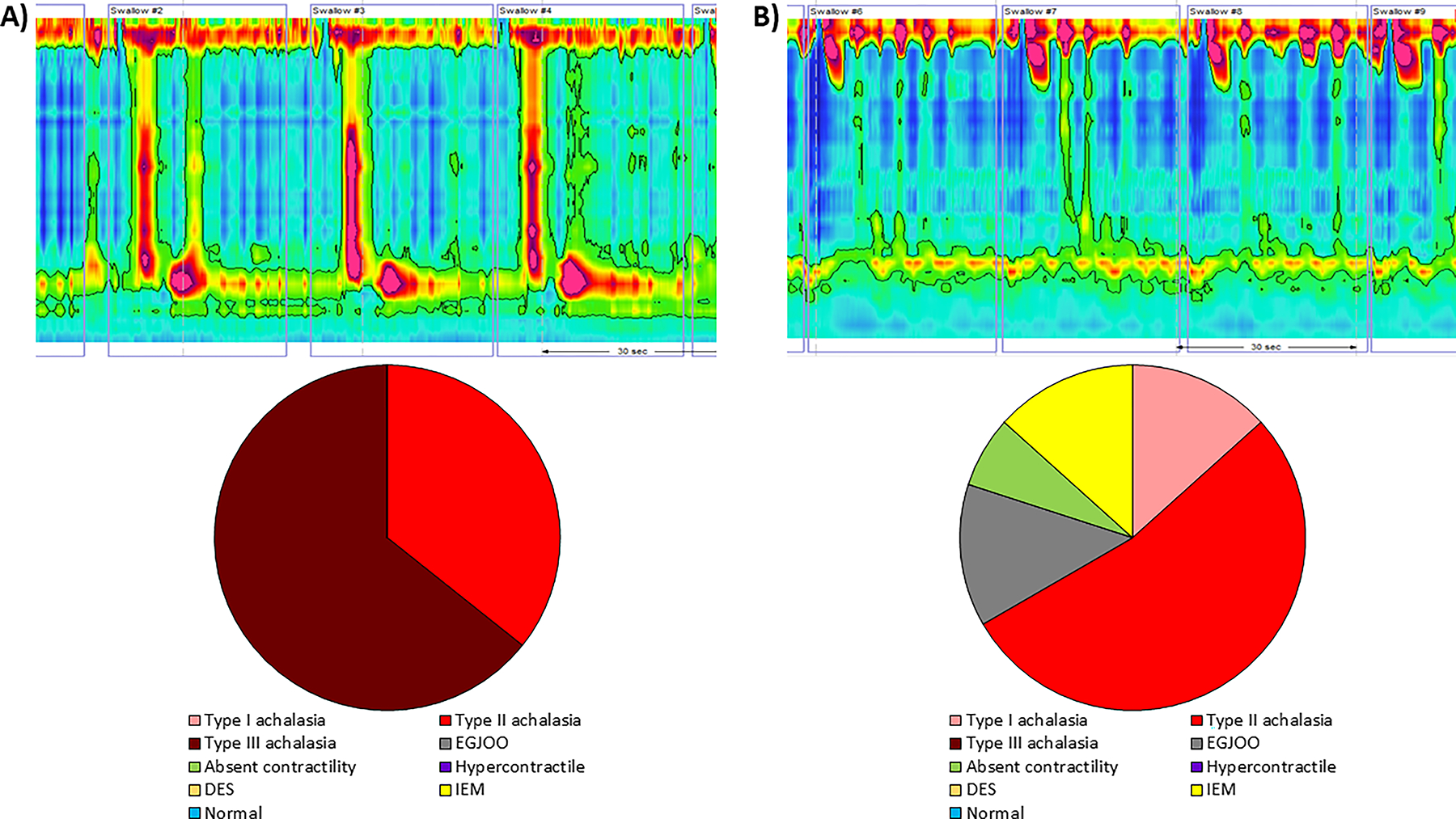
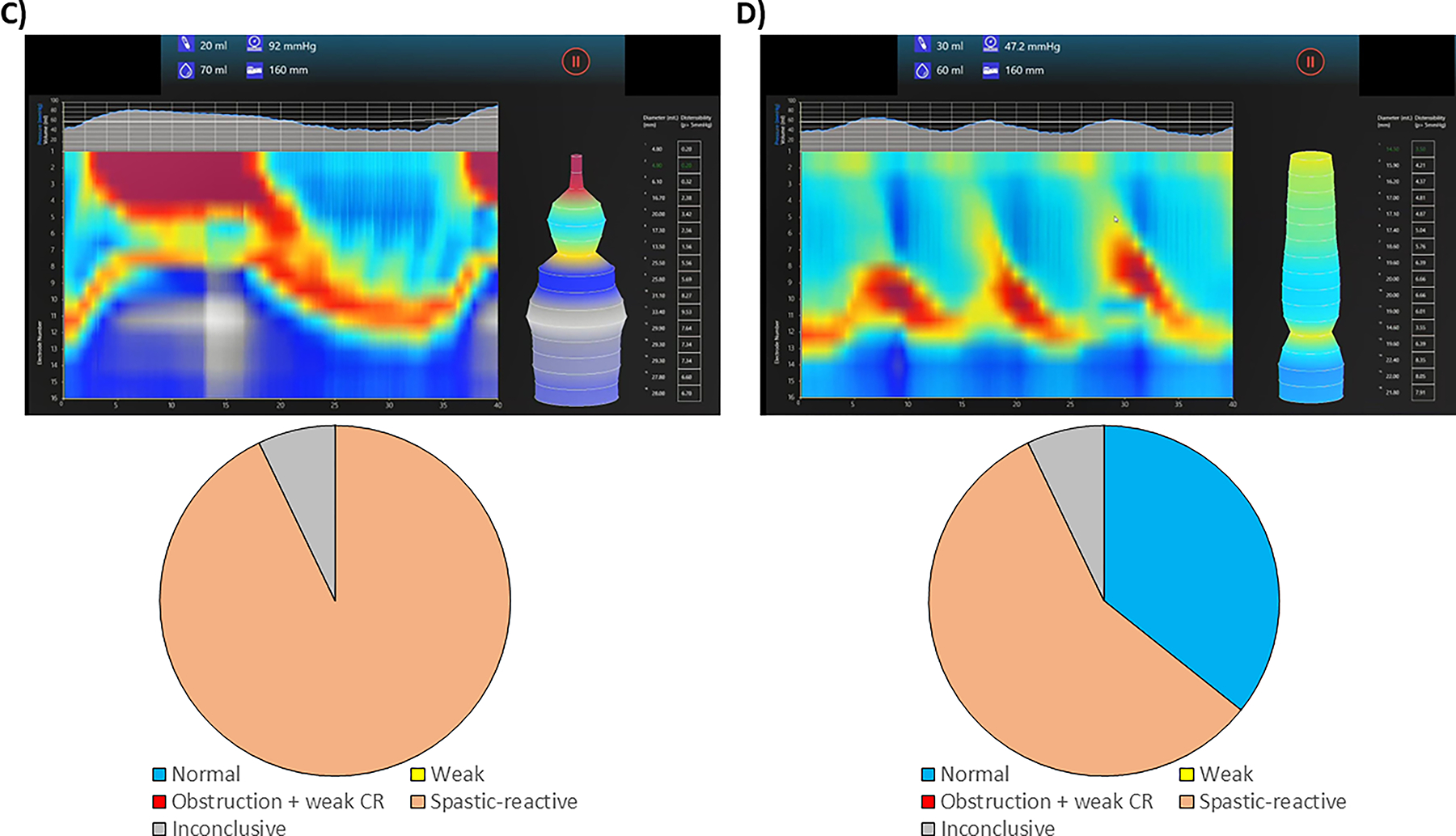
Methods: Esophageal motility specialists from multiple institutions completed the interpretation of 40 consecutive HRM and 40 FLIP studies. Interrater agreement was assessed using intraclass correlation coefficient (ICC) for continuous variables and Fleiss' κ statistics for nominal variables. Accuracies of rater interpretation were assessed using the consensus of 3 experienced raters as the reference standard.
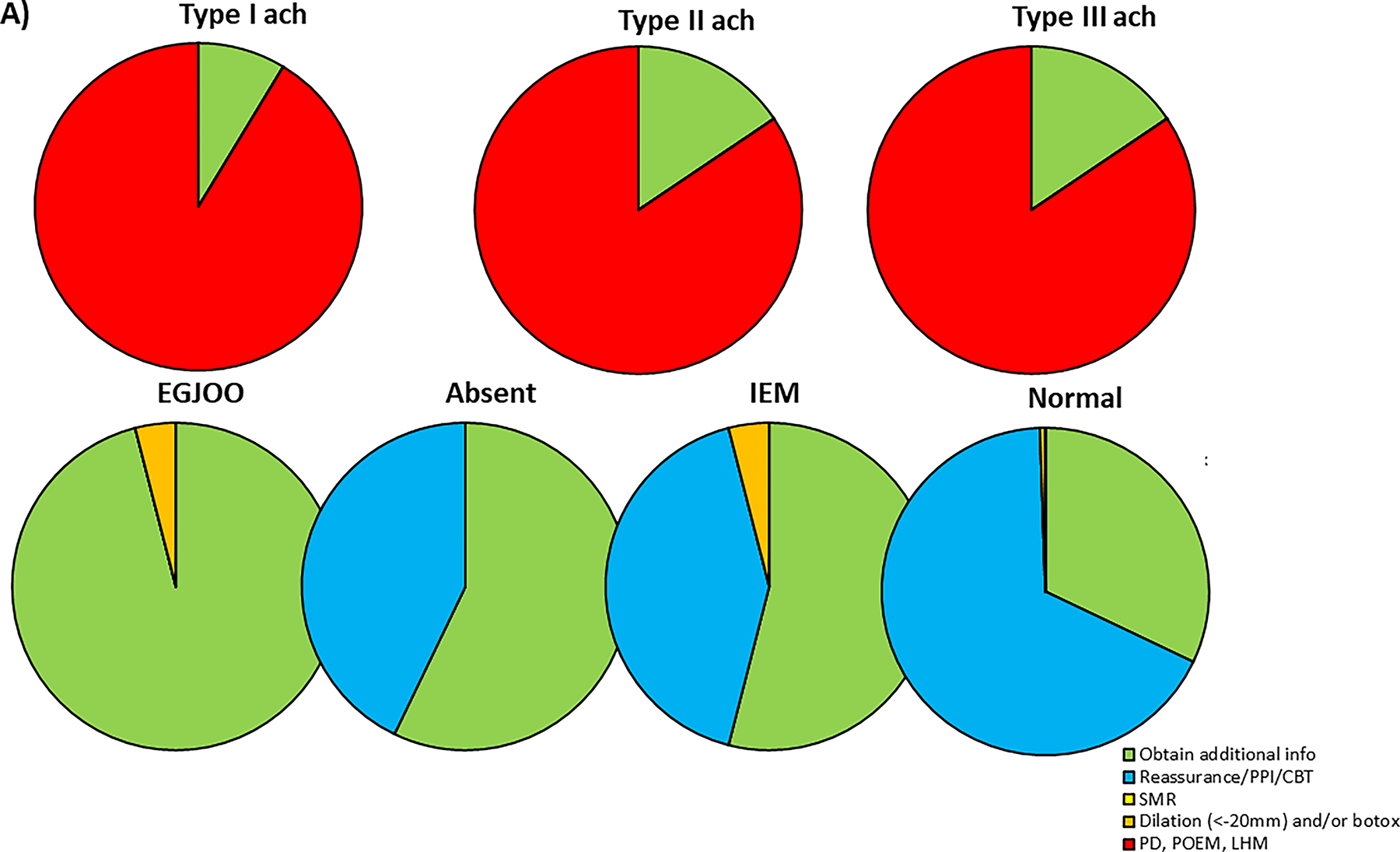
Results: Fifteen raters completed the HRM and FLIP studies. An excellent interrater agreement was seen in supine median integral relaxation pressure (ICC 0.96, 95% confidence interval 0.95-0.98), and a good agreement was seen with the assessment of esophagogastric junction (EGJ) outflow, peristalsis, and assignment of a Chicago Classification version 4.0 diagnosis using HRM (κ = 0.71, 0.75, and 0.70, respectively). An excellent interrater agreement for EGJ distensibility index and maximum diameter (0.91 [0.90-0.94], 0.92 [0.89-0.95]) was seen, and a moderate-to-good agreement was seen in the assignment of EGJ opening classification, contractile response pattern, and motility classification (κ = 0.68, 0.56, and 0.59, respectively) on FLIP. Rater accuracy for Chicago Classification version 4.0 diagnosis on HRM was 82% (95% confidence interval 78%-84%) and for motility diagnosis on FLIP Panometry was 78% (95% confidence interval 72%-81%).
Discussion: Our study demonstrates high levels of interrater agreement and accuracy in the interpretation of HRM and FLIP metrics and moderate-to-high levels for motility classification in FLIP, supporting the use of these approaches for primary or complementary evaluation of esophageal motility disorders.
Copyright © 2023 by The American College of Gastroenterology.
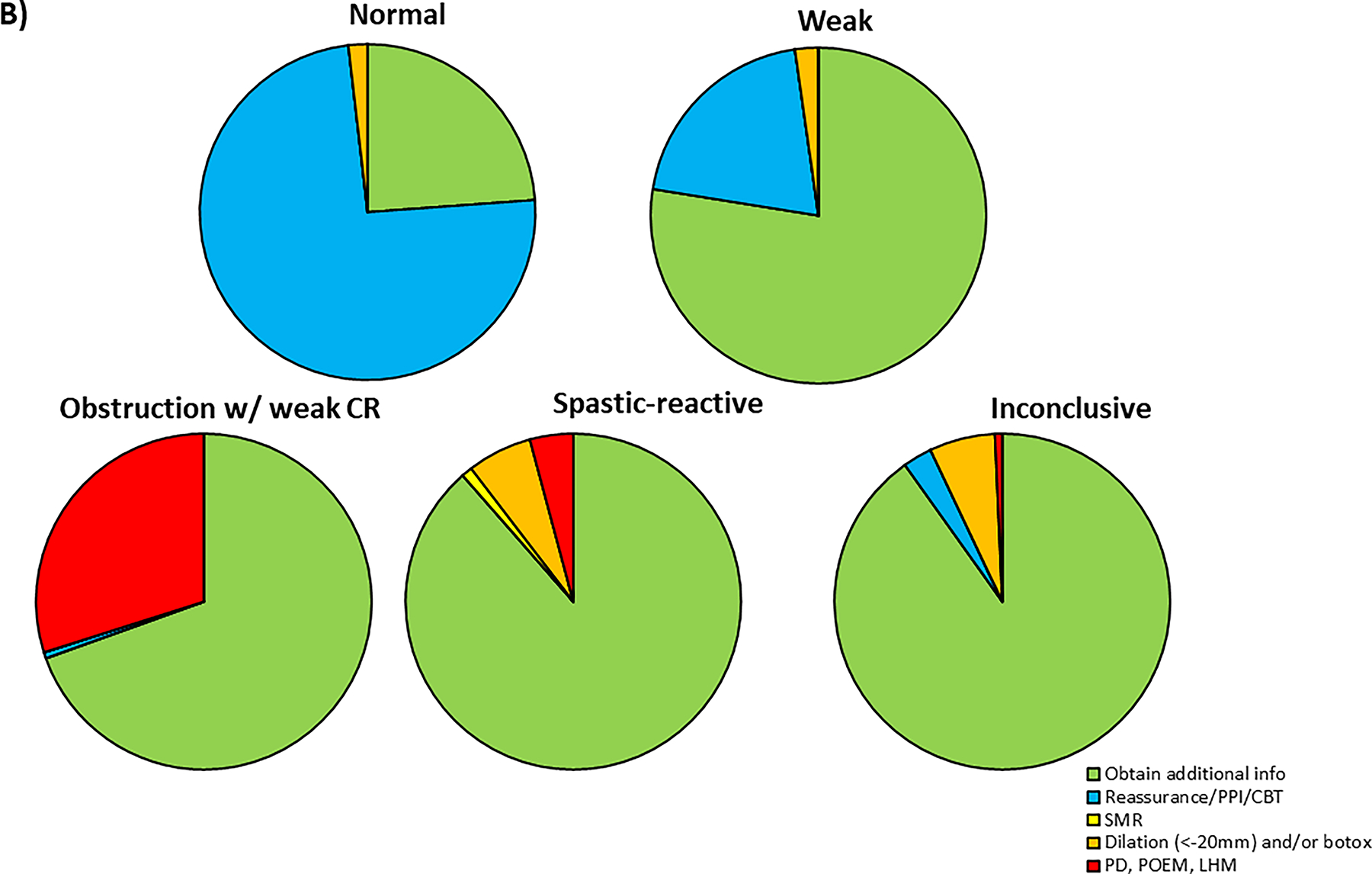
Figures