

Residual Risk of Breast Cancer After Bariatric Surgery
- PMID: 37043196
- PMCID: PMC10099105
- DOI: 10.1001/jamasurg.2023.0530
Residual Risk of Breast Cancer After Bariatric Surgery
Abstract
Importance: Excess adiposity confers higher risk of breast cancer for women. For women who have lost substantial weight, it is unclear whether previous obesity confers residual increased baseline risk of breast cancer compared with peers without obesity.
Objectives: To determine whether there is a residual risk of breast cancer due to prior obesity among patients who undergo bariatric surgery.
Design, setting, and participants: Retrospective matched cohort study of 69 260 women with index date between January 1, 2010, and December 31, 2016. Patients were followed up for 5 years after bariatric surgery or index date. Population-based clinical and administrative data from multiple databases in Ontario, Canada, were used to match a cohort of women who underwent bariatric surgery for obesity (baseline body mass index [BMI] ≥35 with comorbid conditions or BMI ≥40) to women without a history of bariatric surgery according to age and breast cancer screening history. Nonsurgical controls were divided into 4 BMI categories (<25, 25-29, 30-34, and ≥35). Data were analyzed on October 21, 2021.
Exposures: Weight loss via bariatric surgery.
Main outcomes and measures: Residual hazard of breast cancer after washout periods of 1, 2, and 5 years. Comparisons were made between the surgical and nonsurgical cohorts overall and within each of the BMI subgroups.
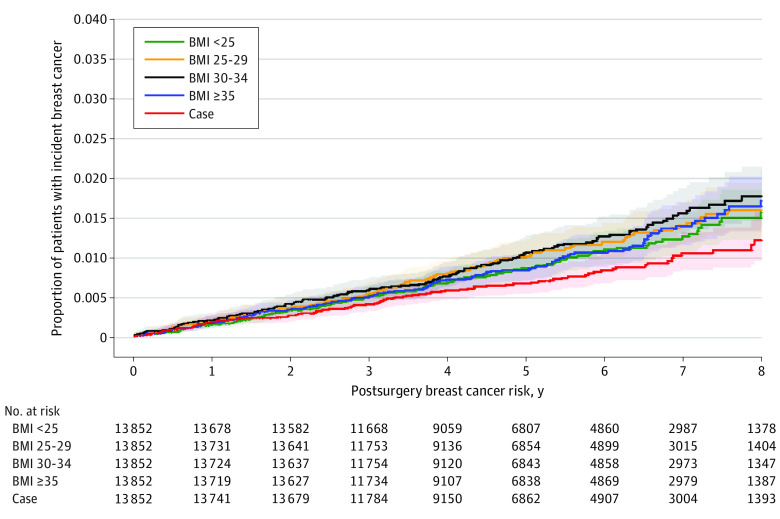
Results: In total, 69 260 women were included in the analysis, with 13 852 women in each of the 5 study cohorts. The mean (SD) age was 45.1 (10.9) years. In the postsurgical cohort vs the overall nonsurgical cohort (n = 55 408), there was an increased hazard for incident breast cancer in the nonsurgical group after washout periods of 1 year (hazard ratio [HR], 1.40 [95% CI, 1.18-1.67]), 2 years (HR, 1.31 [95% CI, 1.12-1.53]), and 5 years (HR, 1.38 [95% CI, 1.21-1.58]). When the postsurgical cohort was compared with the nonsurgical cohort with BMI less than 25, the hazard of incident breast cancer was not significantly different regardless of the washout period, whereas there was a reduced hazard for incident breast cancer among postsurgical patients compared with nonsurgical patients in all high BMI categories (BMI ≥25).
Conclusions and relevance: Findings suggest that bariatric surgery was associated with a reduced risk of developing breast cancer for women with prior obesity equivalent to that of a woman with a BMI less than 25 and a lower risk when compared with all groups with BMI greater than or equal to 25.
Conflict of interest statement
Figures
Comment in
-
Bariatric Surgery for Breast Cancer Risk Reduction-Benefit May Not Be One Size Fits All.JAMA Surg. 2023 Jun 1;158(6):641-642. doi: 10.1001/jamasurg.2023.0534. JAMA Surg. 2023. PMID: 37043229 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
