

A Consideration of Optimal Head Position in Transsylvian Selective Amygdalohippocampectomy
- PMID: 37045769
- PMCID: PMC10406460
- DOI: 10.2176/jns-nmc.2022-0283
A Consideration of Optimal Head Position in Transsylvian Selective Amygdalohippocampectomy
Abstract
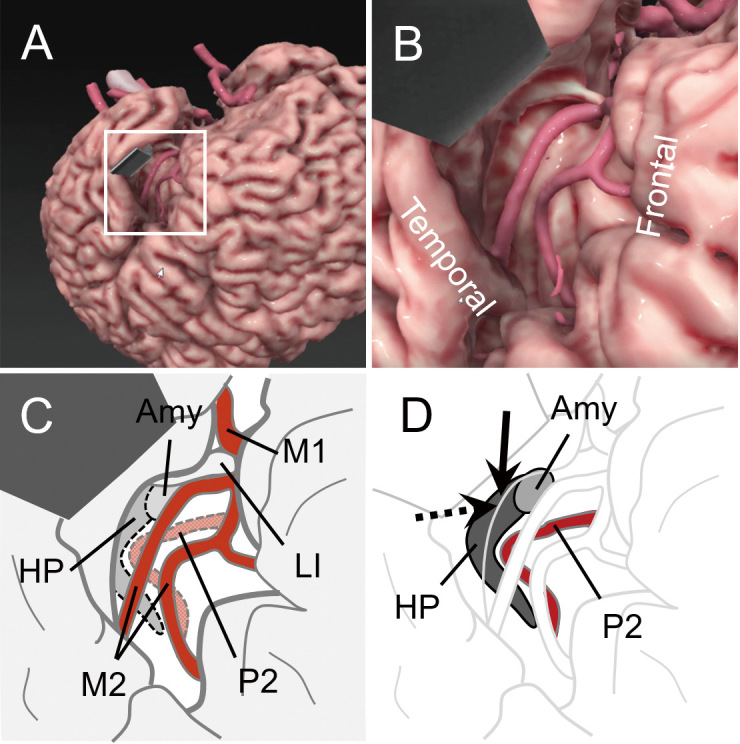
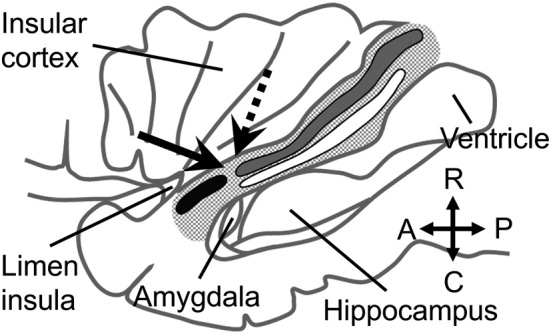
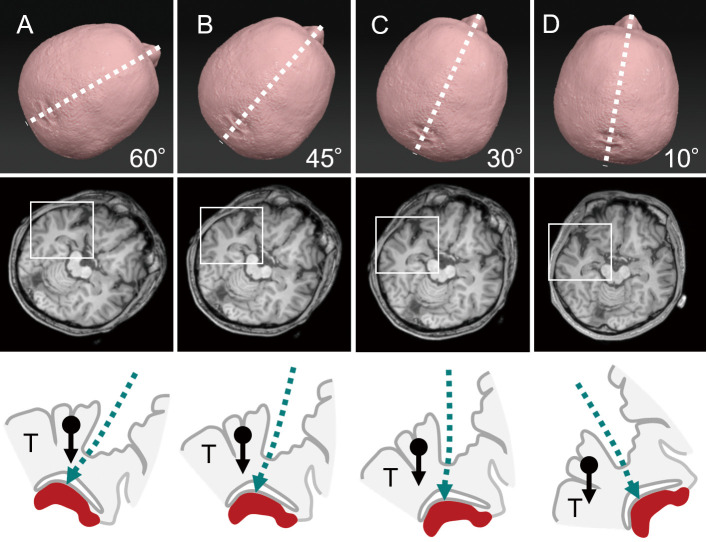
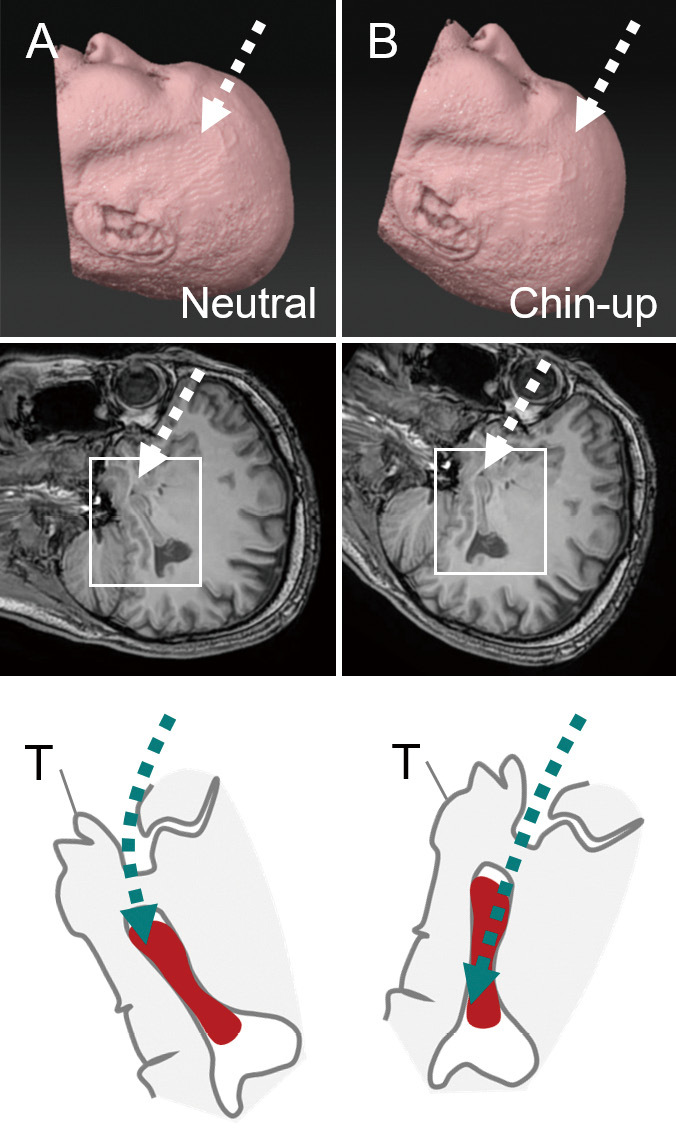
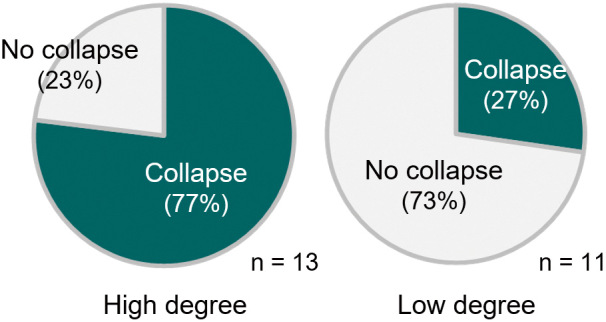
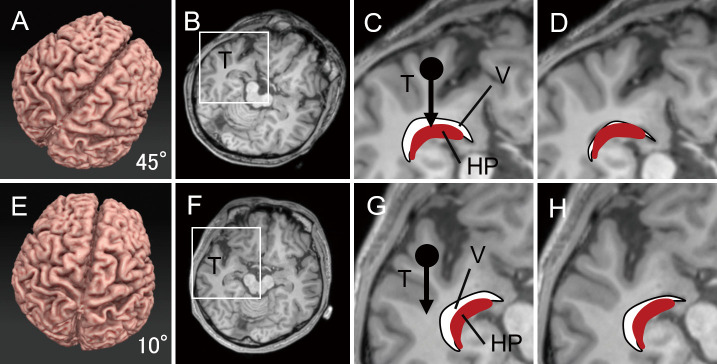
Transsylvian selective amygdalohippocampectomy (TSA) is one of the predominant surgical options for drug-resistant mesial temporal lobe epilepsy. The purpose of this article is to highlight the unique features of TSA and determine the setting to perform safe and secure TSA with special reference to the optimal head position. TSA should be performed via a small surgical corridor in the temporal stem that contains functionally important fiber tracts, including the uncinate fasciculus, the inferior fronto-occipital fasciculus, and the optic radiation. Graphical simulations proposed that low-degree (<30°) head rotation had the advantage of sufficiently opening the surgical field in TSA and may help surgical procedures within the limited exposure of the medial temporal structures. Inspection of the surgical videos implied that the collapse of the inferior horn was prevented in low-degree rotation, probably because the deformation due to the brain shift was minimized in the medial temporal structures. A simulation also implied that chin-up position had the advantage of resecting the tail of the hippocampus in a straightforward manner. We suggest that the setting is optimized in TSA with low-degree rotation and chin-up head position.
Keywords: amygdalohippocampectomy; anterior temporal lobectomy; head position; lateral ventricle; mesial temporal lobe epilepsy.
Conflict of interest statement
The authors declare no conflict of interest related to this work.
Figures
References
-
- Yaşargil MG, Teddy PJ, Roth P: Selective Amygdalo-hippocampectomy: operative anatomy and surgical technique. In: Advances and Technical Standards in Neurosurgery. Vol 12. Symon L, Brihaye J, Guidetti B, et al. , Eds. Springer-Verlag, Wien, New York, 1985: 93-123 - PubMed
-
- Morino M: Selective amygdalohippocampectomy. In: Microsurgery of Intractable Epilepsy. Morino M, Ed. Medical View Co., Ltd., Tokyo, 2013: 16-26
-
- Yonekawa Y: [Operative neurosurgery: personal view and historical backgrounds (4). Selective amygdalohippocampectomy SAHE]. No Shinkei Geka 35: 1183-1196, 2007(Japanese) - PubMed
-
- Helmstaedter C, Richter S, Roske S, Oltmanns F, Schramm J, Lehmann TN: Differential effects of temporal pole resection with amygdalohippocampectomy versus selective amygdalohippocampectomy on material-specific memory in patients with mesial temporal lobe epilepsy. Epilepsia 49: 88-97, 2008 - PubMed