

Low cancer yield in PI-RADS 3 upgraded to 4 by dynamic contrast-enhanced MRI: is it time to reconsider scoring categorization?
- PMID: 37045981
- PMCID: PMC10326099
- DOI: 10.1007/s00330-023-09605-0
Low cancer yield in PI-RADS 3 upgraded to 4 by dynamic contrast-enhanced MRI: is it time to reconsider scoring categorization?
Abstract
Objectives: To evaluate MRI diagnostic performance in detecting clinically significant prostate cancer (csPCa) in peripheral-zone PI-RADS 4 lesions, comparing those with clearly restricted diffusion (DWI-score 4), and those with equivocal diffusion pattern (DWI-score 3) and positive dynamic contrast-enhanced (DCE) MRI.
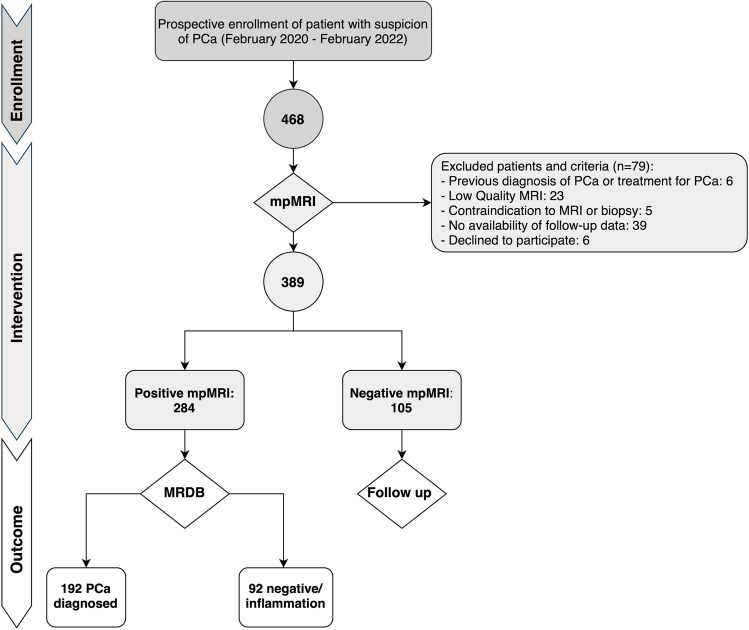
Methods: This observational prospective study enrolled 389 men referred to MRI and, if positive (PI-RADS 3 with PSA-density [PSAD] ≥ 0.15 ng/mL/mL, 4 and 5), to MRI-directed biopsy. Lesions with DWI-score 3 and positive DCE were classified as "PI-RADS 3up," instead of PI-RADS 4. Univariable and multivariable analyses were implemented to determine features correlated to csPCa detection.
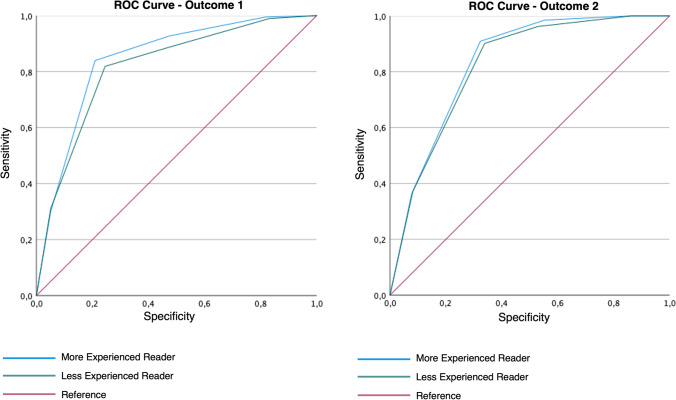
Results: Prevalence of csPCa was 14.5% and 53.3% in PI-RADS categories 3up and 4, respectively (p < 0.001). MRI showed a sensitivity of 100.0%, specificity 40.9%, PPV 46.5%, NPV 100.0%, and accuracy 60.9% for csPCa detection. Modifying the threshold to consider MRI positive and to indicate biopsy (same as previously described, but PI-RADS 3up only when associated with elevated PSAD), the sensitivity changed to 93.9%, specificity 57.2%, PPV 53.0%, NPV 94.8%, and accuracy 69.7%. Age (p < 0.001), PSAD (p < 0.001), positive DWI (p < 0.001), and PI-RADS score (p = 0.04) resulted in independent predictors of csPCa.
Conclusions: Most cases of PI-RADS 3up were false-positives, suggesting that upgrading peripheral lesions with DWI-score 3 to PI-RADS 4 because of positive DCE has a detrimental effect on MRI accuracy, decreasing the true prevalence of csPCa in the PI-RADS 4 category. PI-RADS 3up should not be upgraded and directed to biopsy only if associated with increased PSAD.
Key points: • As per PI-RADS v2.1 recommendations, in case of a peripheral zone lesion with equivocal diffusion-weighted imaging (DWI score 3), but positive dynamic contrast-enhanced (DCE) MRI, the overall PI-RADS score should be upgraded to 4. • The current PI-RADS recommendation of upgrading PI-RADS 3 lesions of the peripheral zone to PI-RADS 4 because of positive DCE decreased clinically significant prostate cancer detection rate in our series. • According to our results, the most accurate threshold for setting indication to prostate biopsy is PI-RADS 3 or PI-RADS 3 with positive DCE both associated with increased PSA density.
Keywords: Biopsy; Multiparametric magnetic resonance imaging; Prostatic neoplasms.
© 2023. The Author(s).
Conflict of interest statement
R. Girometti is a Deputy Editor of European Radiology. He has not taken part in the review or selection process of this article.
V. Panebianco is a member of the European Radiology Scientific Editorial Board. She has not taken part in the review or selection process of this article.
The remaining authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
Comment in
-
Are upgraded DCE-positive PI-RADS 3 lesions truly suspicious for clinically significant prostate cancer?Eur Radiol. 2023 Aug;33(8):5825-5827. doi: 10.1007/s00330-023-09711-z. Epub 2023 May 8. Eur Radiol. 2023. PMID: 37154954 No abstract available.
Similar articles
-
Investigating the role of DCE-MRI, over T2 and DWI, in accurate PI-RADS v2 assessment of clinically significant peripheral zone prostate lesions as defined at radical prostatectomy.Abdom Radiol (NY). 2019 Apr;44(4):1520-1527. doi: 10.1007/s00261-018-1807-6. Abdom Radiol (NY). 2019. PMID: 30361870 Free PMC article.
-
Prevalence of Prostate Cancer in PI-RADS Version 2.1 Transition Zone Atypical Nodules Upgraded by Abnormal DWI: Correlation With MRI-Directed TRUS-Guided Targeted Biopsy.AJR Am J Roentgenol. 2021 Mar;216(3):683-690. doi: 10.2214/AJR.20.23932. Epub 2021 Jan 21. AJR Am J Roentgenol. 2021. PMID: 32755208
-
Head-to-head comparison of biparametric versus multiparametric MRI of the prostate before robot-assisted transperineal fusion prostate biopsy.World J Urol. 2022 Oct;40(10):2431-2438. doi: 10.1007/s00345-022-04120-1. Epub 2022 Aug 4. World J Urol. 2022. PMID: 35922717 Free PMC article.
-
Magnetic Resonance Imaging, Clinical, and Biopsy Findings in Suspected Prostate Cancer: A Systematic Review and Meta-Analysis.JAMA Netw Open. 2024 Mar 4;7(3):e244258. doi: 10.1001/jamanetworkopen.2024.4258. JAMA Netw Open. 2024. PMID: 38551559 Free PMC article.
-
Current Status of Biparametric MRI in Prostate Cancer Diagnosis: Literature Analysis.Life (Basel). 2022 May 28;12(6):804. doi: 10.3390/life12060804. Life (Basel). 2022. PMID: 35743835 Free PMC article. Review.
Cited by
-
Interpreting Prostate MRI Reports in the Era of Increasing Prostate MRI Utilization: A Urologist's Perspective.Diagnostics (Basel). 2024 May 20;14(10):1060. doi: 10.3390/diagnostics14101060. Diagnostics (Basel). 2024. PMID: 38786358 Free PMC article. Review.
-
Design of a magnetic resonance imaging-based screening program for early diagnosis of prostate cancer: preliminary results of a randomized controlled trial-Prostate Cancer Secondary Screening in Sapienza (PROSA).Eur Radiol. 2024 Jan;34(1):204-213. doi: 10.1007/s00330-023-10019-1. Epub 2023 Aug 10. Eur Radiol. 2024. PMID: 37561183 Clinical Trial.
-
Prospective evaluation of mpMRI-derived nomograms for detecting prostate cancer in PI-RADS v2.1 upgraded and non-upgraded lesions.Front Oncol. 2025 Jun 4;15:1510049. doi: 10.3389/fonc.2025.1510049. eCollection 2025. Front Oncol. 2025. PMID: 40535126 Free PMC article.
-
Nomograms for predicting clinically significant prostate cancer in men with PI-RADS-3 biparametric magnetic resonance imaging.Am J Cancer Res. 2024 Jan 15;14(1):73-85. doi: 10.62347/XBBI9870. eCollection 2024. Am J Cancer Res. 2024. PMID: 38323293 Free PMC article.
-
Evaluating Biparametric Versus Multiparametric Magnetic Resonance Imaging for Diagnosing Clinically Significant Prostate Cancer: An International, Paired, Noninferiority, Confirmatory Observer Study.Eur Urol. 2025 Feb;87(2):240-250. doi: 10.1016/j.eururo.2024.09.035. Epub 2024 Oct 22. Eur Urol. 2025. PMID: 39438187 Free PMC article.
References
-
- Sathianathen NJ, Omer A, Harriss E, et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant prostate cancer in the prostate imaging reporting and data system era: a systematic review and meta-analysis. Eur Urol. 2020;78:402–414. doi: 10.1016/j.eururo.2020.03.048. - DOI - PubMed
-
- Sciarra A, Panebianco V, Cattarino S, et al. Multiparametric magnetic resonance imaging of the prostate can improve the predictive value of the urinary prostate cancer antigen 3 test in patients with elevated prostate-specific antigen levels and a previous negative biopsy. BJU Int. 2012;110:1661–1665. doi: 10.1111/j.1464-410X.2012.11146.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
