

Clonal haematopoiesis and risk of chronic liver disease
- PMID: 37046084
- PMCID: PMC10405350
- DOI: 10.1038/s41586-023-05857-4
Clonal haematopoiesis and risk of chronic liver disease
Erratum in
-
Author Correction: Clonal haematopoiesis and risk of chronic liver disease.Nature. 2023 Jul;619(7970):E47. doi: 10.1038/s41586-023-06375-z. Nature. 2023. PMID: 37400552 No abstract available.
Abstract
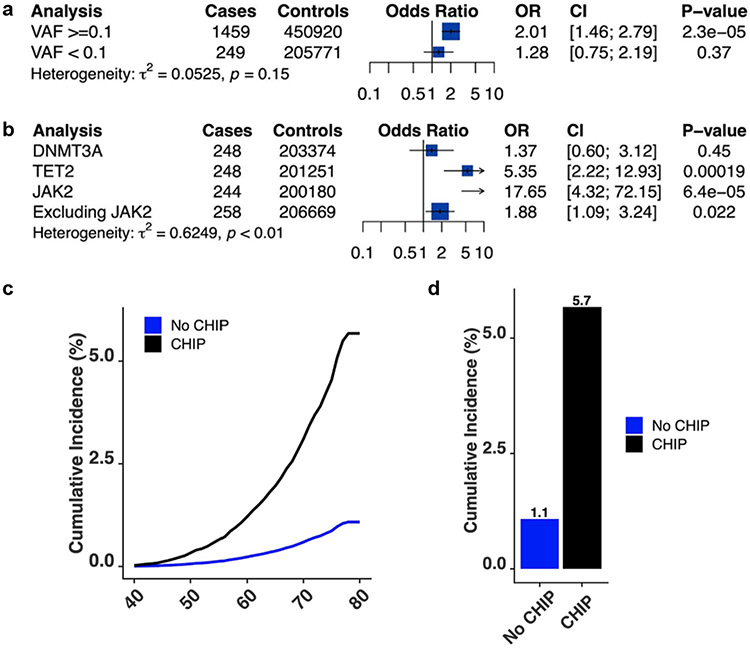
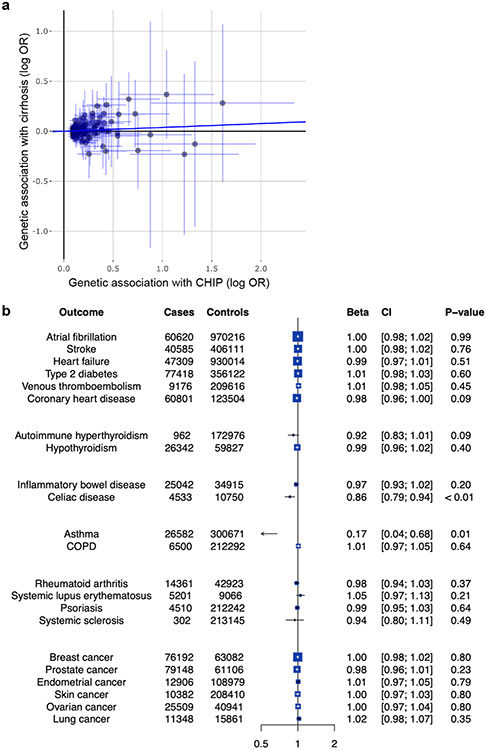
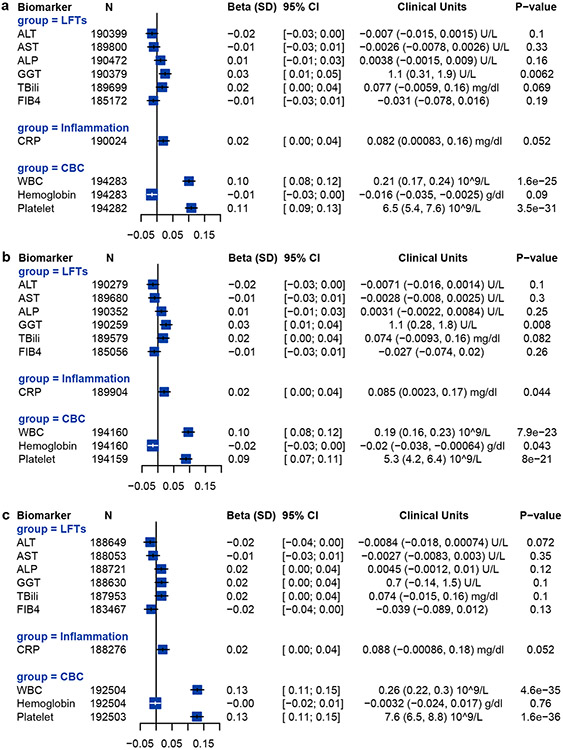
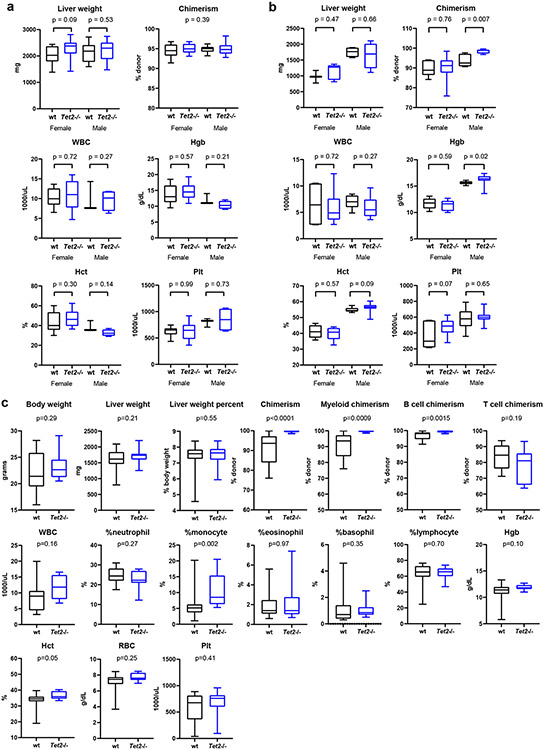
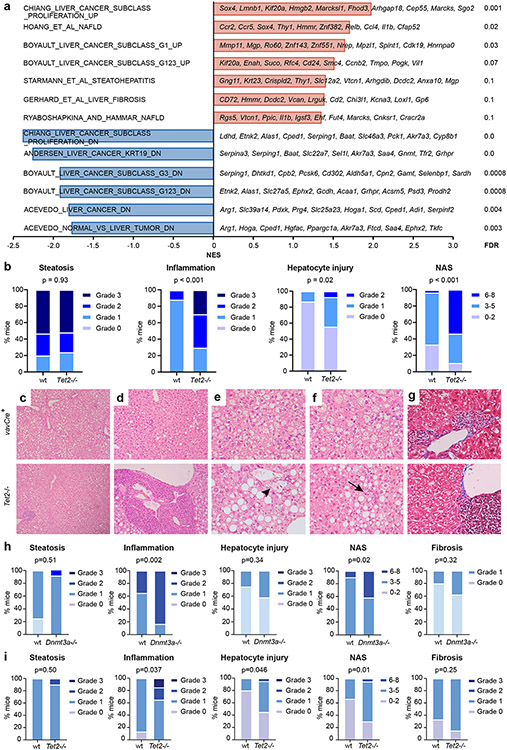
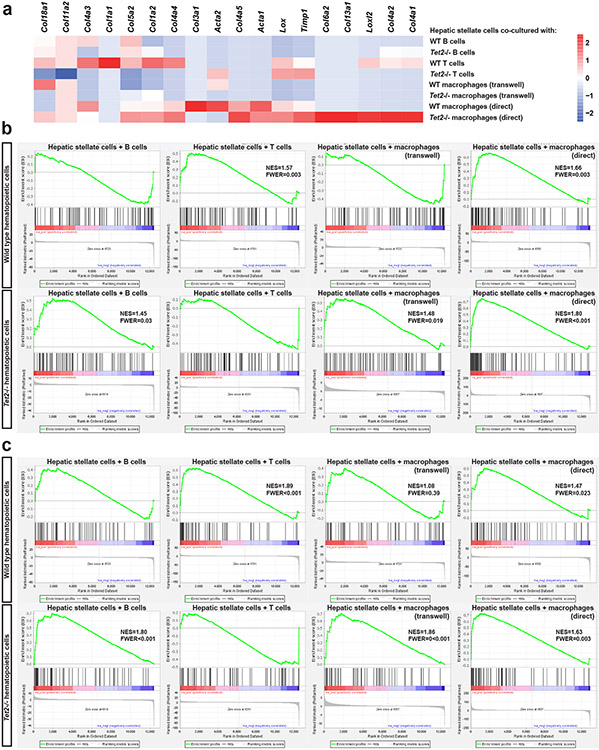
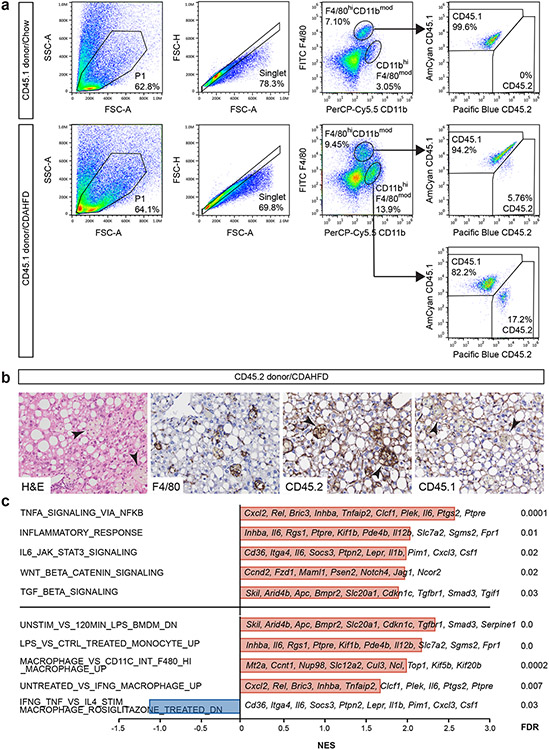
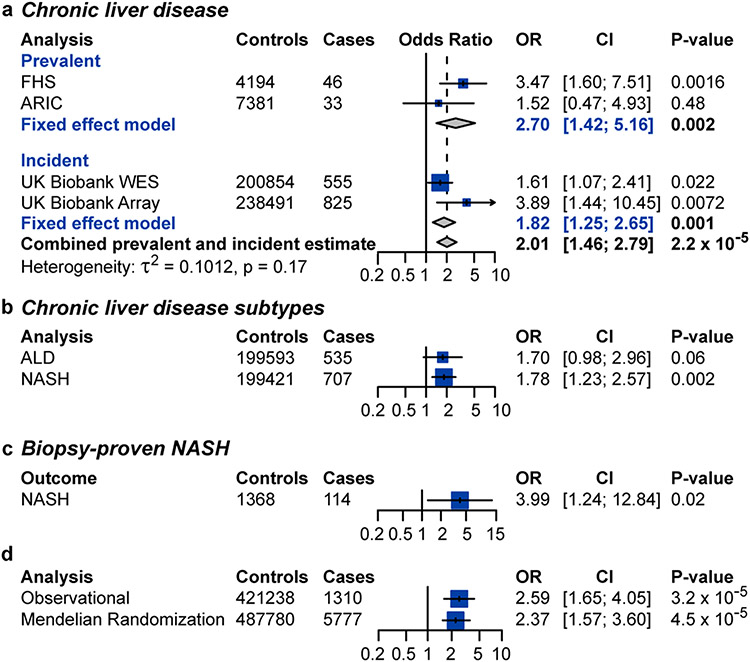
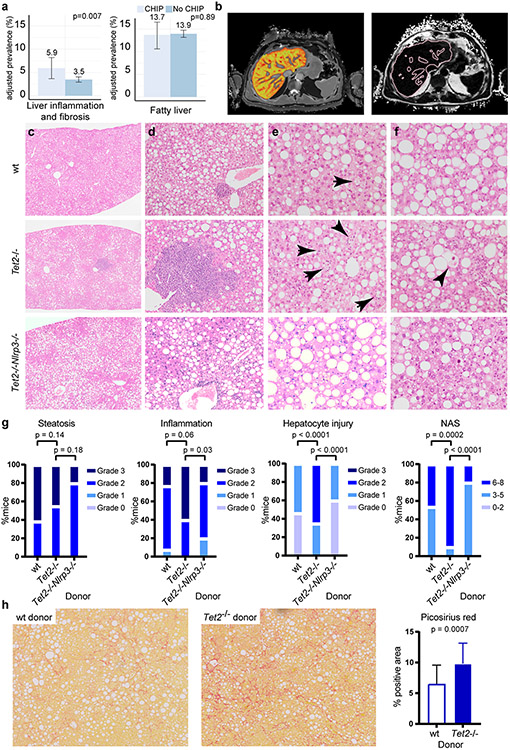
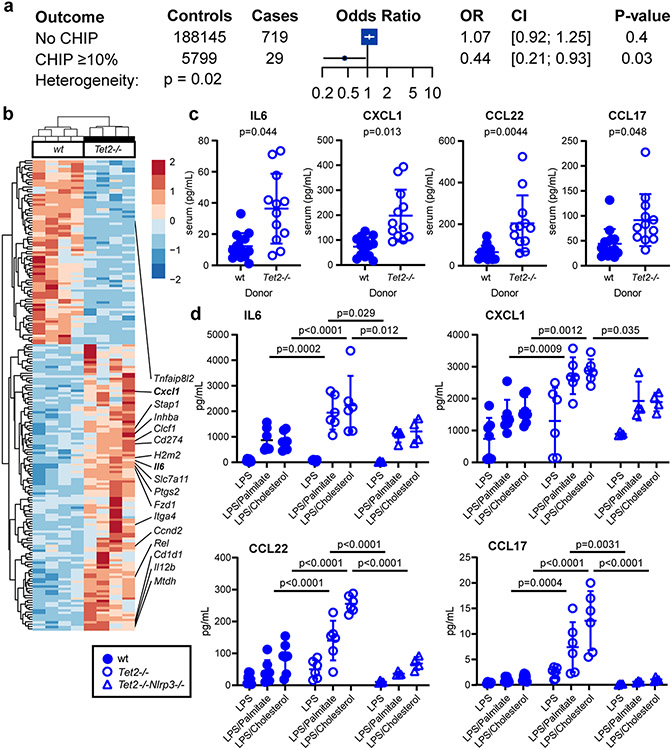
Chronic liver disease is a major public health burden worldwide1. Although different aetiologies and mechanisms of liver injury exist, progression of chronic liver disease follows a common pathway of liver inflammation, injury and fibrosis2. Here we examined the association between clonal haematopoiesis of indeterminate potential (CHIP) and chronic liver disease in 214,563 individuals from 4 independent cohorts with whole-exome sequencing data (Framingham Heart Study, Atherosclerosis Risk in Communities Study, UK Biobank and Mass General Brigham Biobank). CHIP was associated with an increased risk of prevalent and incident chronic liver disease (odds ratio = 2.01, 95% confidence interval (95% CI) [1.46, 2.79]; P < 0.001). Individuals with CHIP were more likely to demonstrate liver inflammation and fibrosis detectable by magnetic resonance imaging compared to those without CHIP (odds ratio = 1.74, 95% CI [1.16, 2.60]; P = 0.007). To assess potential causality, Mendelian randomization analyses showed that genetic predisposition to CHIP was associated with a greater risk of chronic liver disease (odds ratio = 2.37, 95% CI [1.57, 3.6]; P < 0.001). In a dietary model of non-alcoholic steatohepatitis, mice transplanted with Tet2-deficient haematopoietic cells demonstrated more severe liver inflammation and fibrosis. These effects were mediated by the NLRP3 inflammasome and increased levels of expression of downstream inflammatory cytokines in Tet2-deficient macrophages. In summary, clonal haematopoiesis is associated with an elevated risk of liver inflammation and chronic liver disease progression through an aberrant inflammatory response.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Competing interests
W.J.W., C. Emdin, B.L.E. and P.N. are inventors on a US provisional patent application related to this work filed by Massachusetts General Hospital and Dana-Farber Cancer Institute (number 63/116,382, filed 20 November 2020). P.N. reports grant support from Amgen, Apple, AstraZeneca, Boston Scientific and Novartis, and personal fees from Allelica, Apple, AstraZeneca, Blackstone Life Sciences, Foresite Labs, Invitae, Novartis, Roche/Genetech and TenSixteen Bio, is a scientific advisory board member of Esperion Therapeutics, geneXwell and TenSixteen Bio, and reports spousal employment at and equity in Vertex, all distinct from the present work. C. Emdin reports personal fees from Acceleron Pharma, Korro Bio, Navitor Pharma, Nference, Novartis and Third Rock Ventures, all distinct from the present work. B.L.E. has received research financial support from Celgene, Deerfield, Novartis and Calico, and consulting fees from GRAIL, and serves on the scientific advisory boards for Neomorph Therapeutics, Skyhawk Therapeutics and Exo Therapeutics, all distinct from the present work. P.N. and B.L.E. are scientific co-founders of TenSixteen Bio, which focuses on somatic mosaicism and precision medicine. L.D. has received research support from Perspectum Ltd, Pfizer, Lumos Pharma and Recordati, is a MGB Innovation Fellow hosted by Third Rock Ventures (a venture capital firm) and remains full time at MGH during the period of this educational program (anticipated 1 October 2022–30 September 2024); the financial interests of L.D. were reviewed and are managed by MGH and MGB in accordance with their conflict-of-interest policies. M.A. received consulting fees from German Accelerator Life Sciences and is a co-founder of and holds equity in iuvando Health, all unrelated to the present work. R. Banerjee, R.C.N., A.D. and M. Kelly receive salaries from and have stock options in Perspectum and research interests in liver and cardiometabolic disease. S.J. is on advisory boards for Novartis, AVRO Bio and Roche Genentech, is a paid consultant for Foresite Labs, reports speaking fees and an honorarium from GSK, is an equity holder and a scientific advisory board member of Bitterroot Bio, and is a co-founder, equity holder, and scientific advisory board member of TenSixteen Bio. R.T.C. has received grant support to his institution from Abbvie, Boehringer, Gilead, Merck, BMS, Roche, Janssen and GSK all unrelated to the present work. All other authors declare no competing interests.
Figures


Comment in
-
Elucidating the link between clonal haematopoiesis and chronic liver disease.Nat Rev Gastroenterol Hepatol. 2023 Jun;20(6):345. doi: 10.1038/s41575-023-00795-y. Nat Rev Gastroenterol Hepatol. 2023. PMID: 37173571 No abstract available.
References
-
- Anstee QM, Reeves HL, Kotsiliti E, Govaere O & Heikenwalder M From NASH to HCC: current concepts and future challenges. Nat. Rev. Gastroenterol. Hepatol 16, 411–428 (2019). - PubMed
-
- Kisseleva T & Brenner D Molecular and cellular mechanisms of liver fibrosis and its regression. Nat. Rev. Gastroenterol. Hepatol 18, 151–166 (2021). - PubMed
-
- Younossi ZM et al. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 69, 564–568 (2020). - PubMed
-
- Scaglione S. et al. The Epidemiology of Cirrhosis in the United States: A Population-based Study. J. Clin. Gastroenterol 49, 690–696 (2015). - PubMed
Methods references
-
- Chalasani N. et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 67, 328–357 (2018). - PubMed
-
- Kleiner DE et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 41, 1313–1321 (2005). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K08 HL159346/HL/NHLBI NIH HHS/United States
- F30 HL149180/HL/NHLBI NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- G12 MD007597/MD/NIMHD NIH HHS/United States
- P50 CA206963/CA/NCI NIH HHS/United States
- R01 HL139865/HL/NHLBI NIH HHS/United States
- S10 OD026880/OD/NIH HHS/United States
- K23 DK113220/DK/NIDDK NIH HHS/United States
- R01 HL142711/HL/NHLBI NIH HHS/United States
- DP2 HL157540/HL/NHLBI NIH HHS/United States
- DP2 ES030554/ES/NIEHS NIH HHS/United States
- K08 CA263555/CA/NCI NIH HHS/United States
- R01 HL117626/HL/NHLBI NIH HHS/United States
- R35 CA253125/CA/NCI NIH HHS/United States
- P30 ES010126/ES/NIEHS NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- T32 GM136651/GM/NIGMS NIH HHS/United States
- R01 DK125782/DK/NIDDK NIH HHS/United States
- R01 HL148565/HL/NHLBI NIH HHS/United States
- U01 HL120393/HL/NHLBI NIH HHS/United States
- R01 HL082945/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- P01 CA108631/CA/NCI NIH HHS/United States
- R01 AI155140/AI/NIAID NIH HHS/United States
- R01 AI136715/AI/NIAID NIH HHS/United States
- S10 OD030463/OD/NIH HHS/United States
- P01 HL132825/HL/NHLBI NIH HHS/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
