

The evolution of non-small cell lung cancer metastases in TRACERx
- PMID: 37046095
- PMCID: PMC10115651
- DOI: 10.1038/s41586-023-05729-x
The evolution of non-small cell lung cancer metastases in TRACERx
Abstract
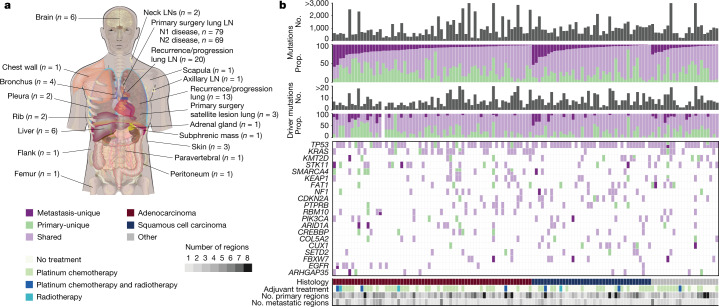
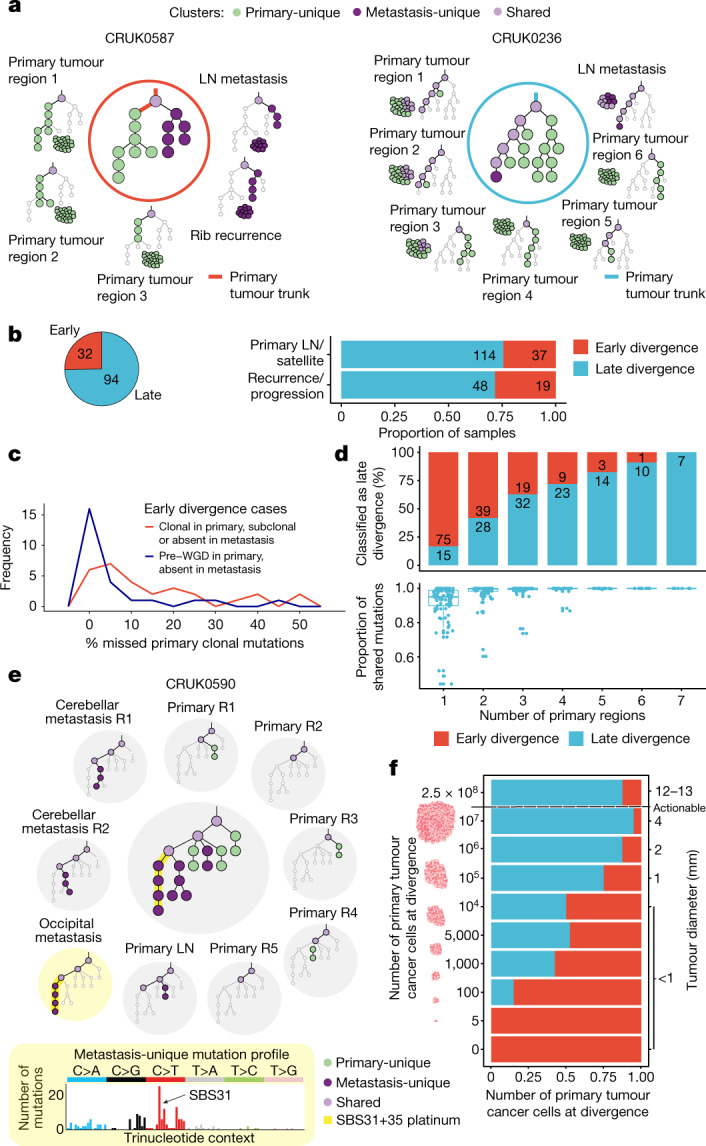
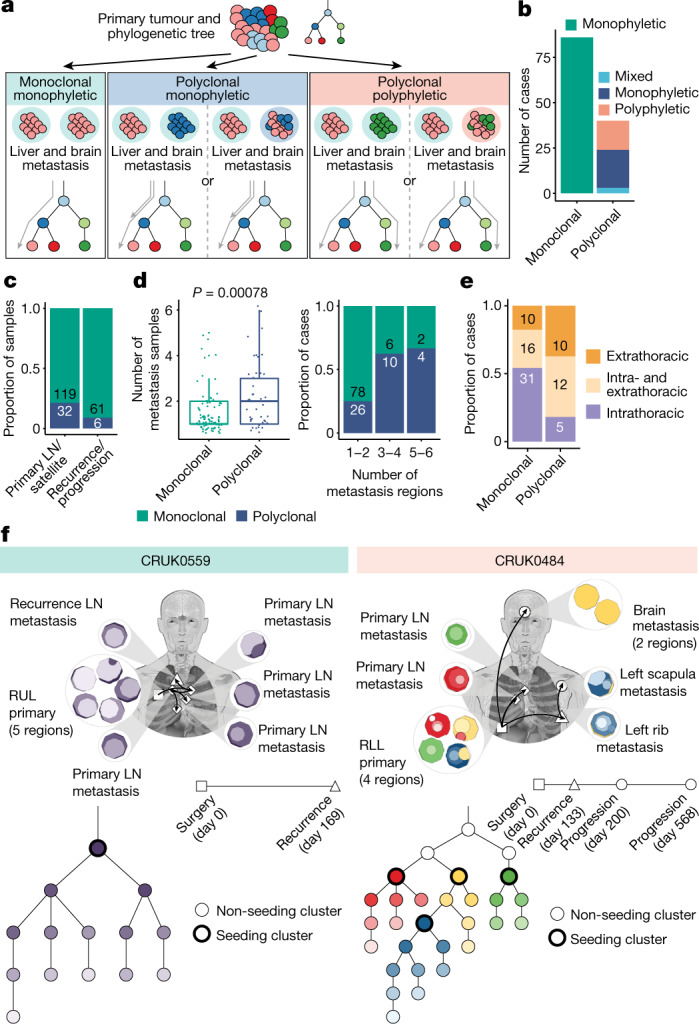
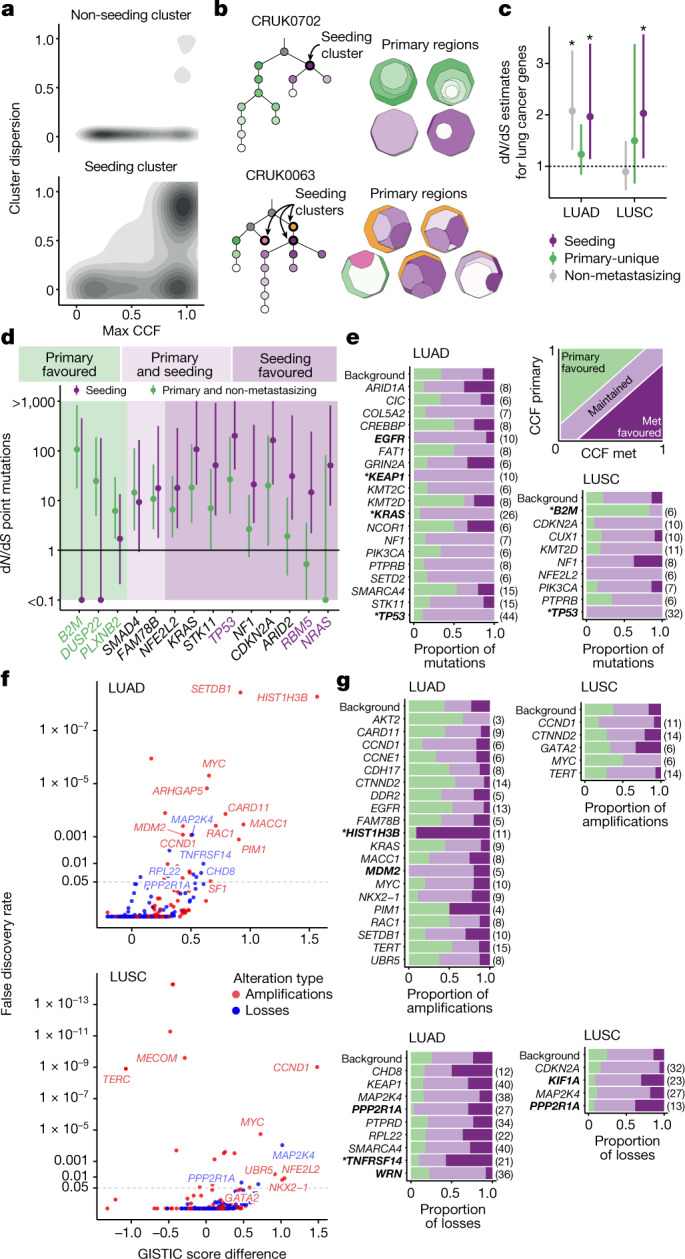
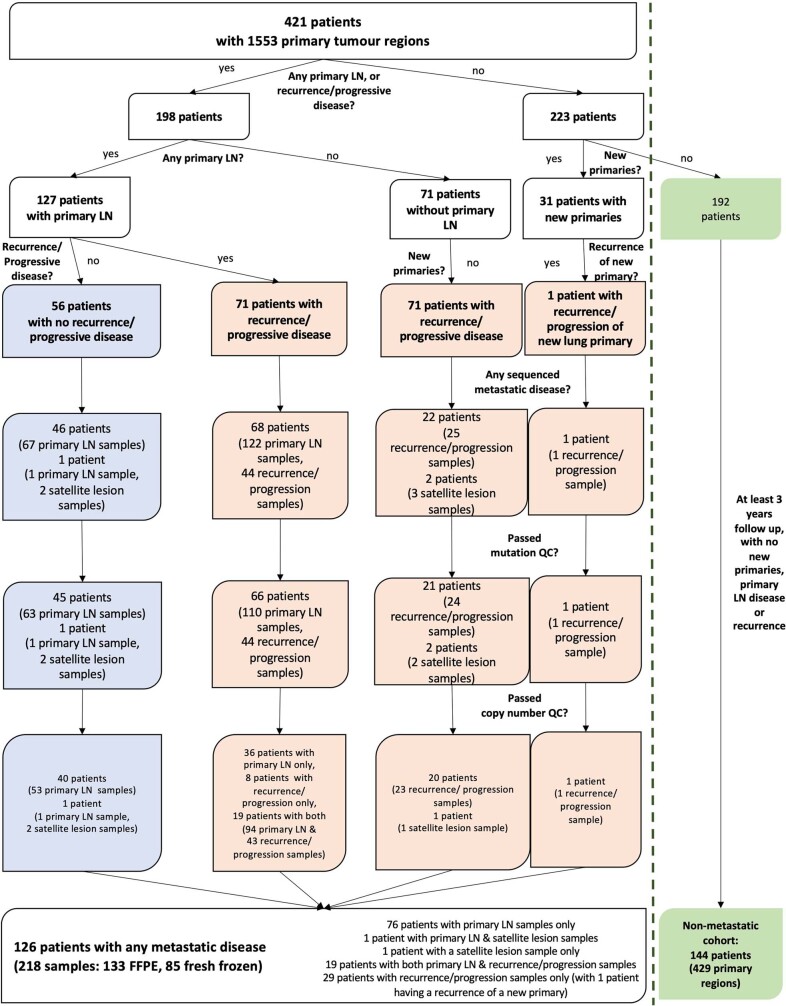
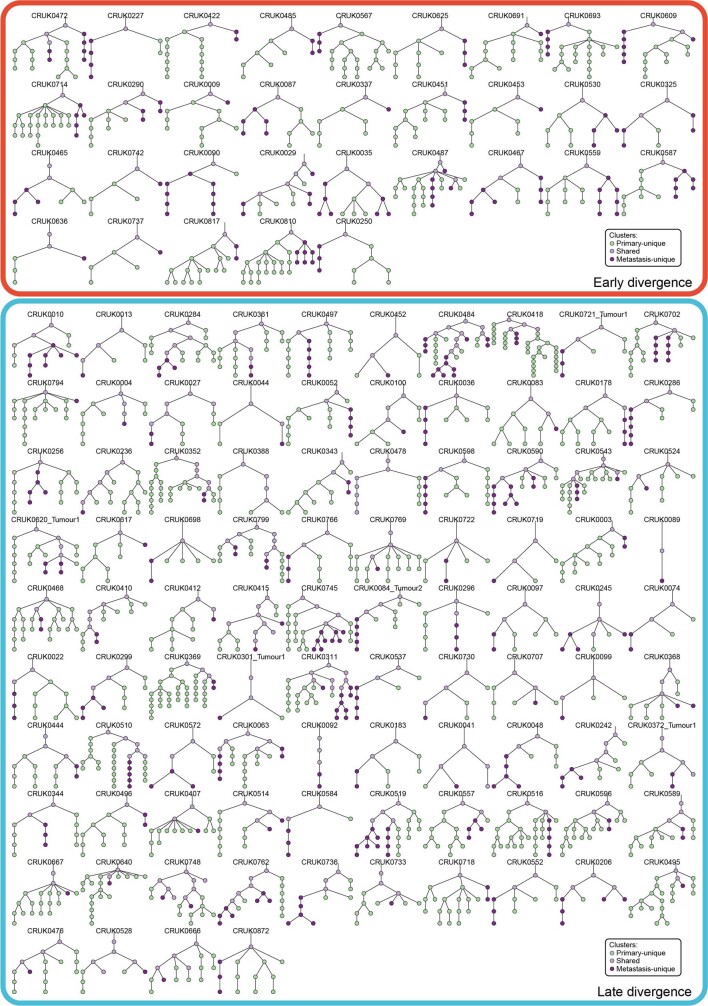
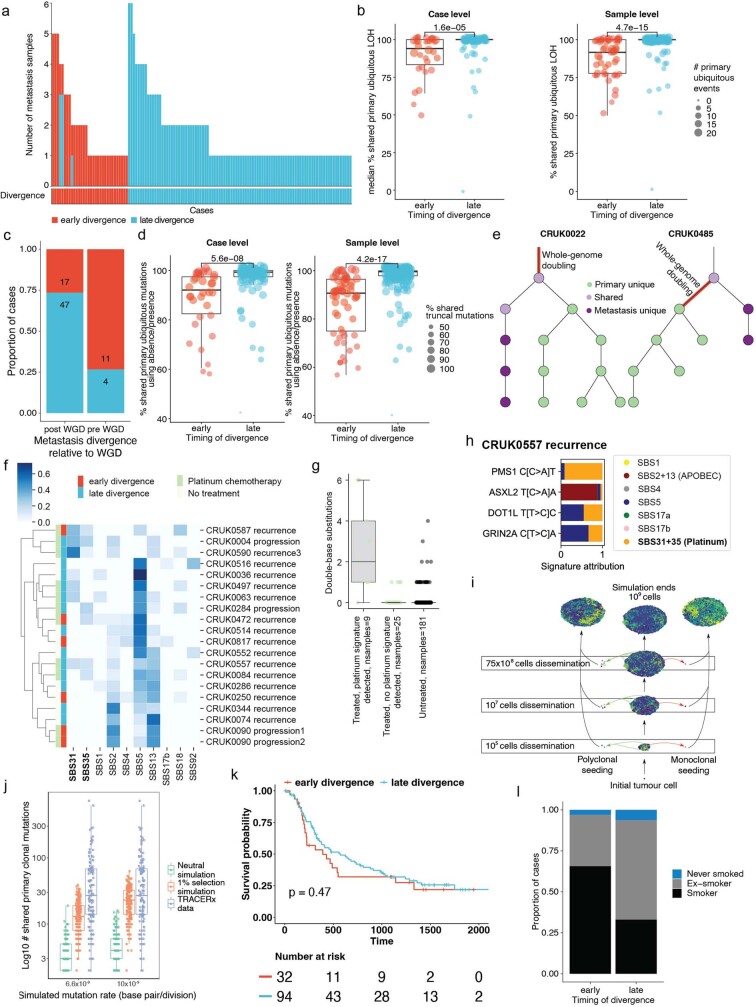
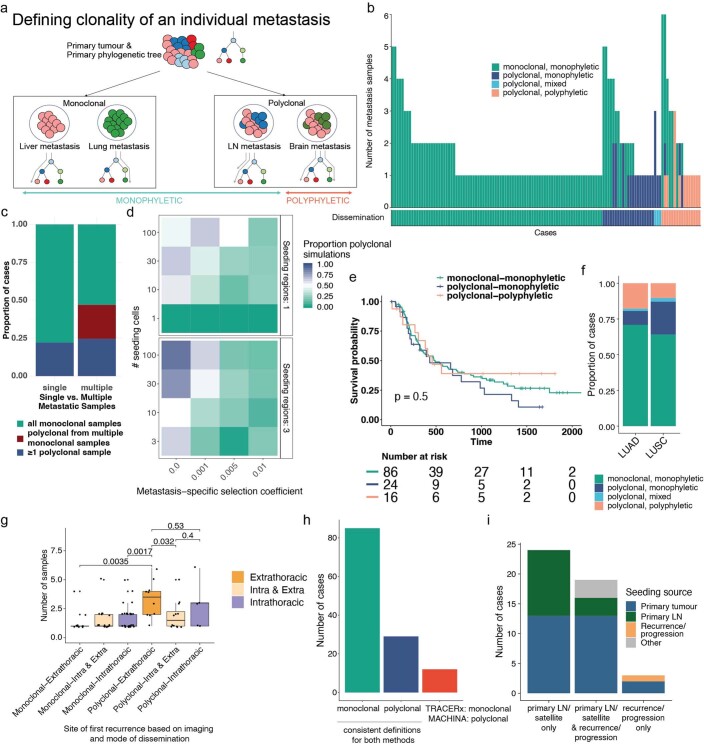
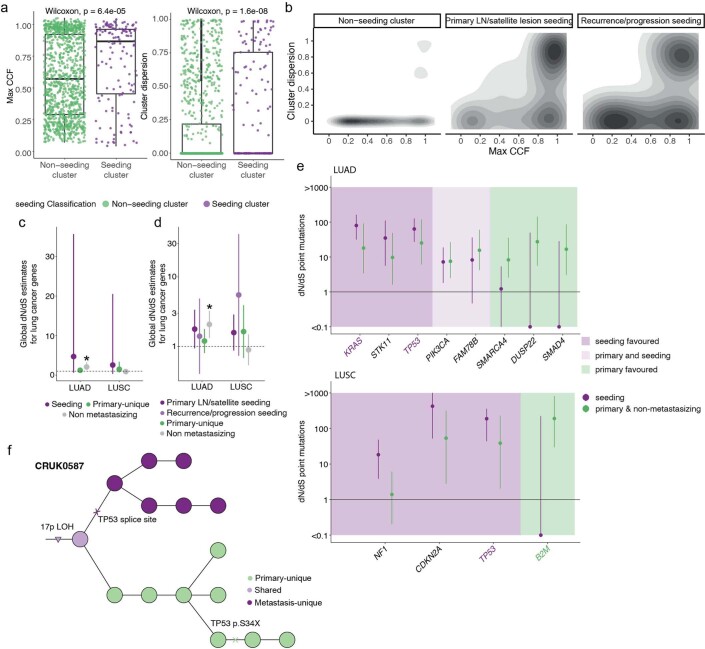
Metastatic disease is responsible for the majority of cancer-related deaths1. We report the longitudinal evolutionary analysis of 126 non-small cell lung cancer (NSCLC) tumours from 421 prospectively recruited patients in TRACERx who developed metastatic disease, compared with a control cohort of 144 non-metastatic tumours. In 25% of cases, metastases diverged early, before the last clonal sweep in the primary tumour, and early divergence was enriched for patients who were smokers at the time of initial diagnosis. Simulations suggested that early metastatic divergence more frequently occurred at smaller tumour diameters (less than 8 mm). Single-region primary tumour sampling resulted in 83% of late divergence cases being misclassified as early, highlighting the importance of extensive primary tumour sampling. Polyclonal dissemination, which was associated with extrathoracic disease recurrence, was found in 32% of cases. Primary lymph node disease contributed to metastatic relapse in less than 20% of cases, representing a hallmark of metastatic potential rather than a route to subsequent recurrences/disease progression. Metastasis-seeding subclones exhibited subclonal expansions within primary tumours, probably reflecting positive selection. Our findings highlight the importance of selection in metastatic clone evolution within untreated primary tumours, the distinction between monoclonal versus polyclonal seeding in dictating site of recurrence, the limitations of current radiological screening approaches for early diverging tumours and the need to develop strategies to target metastasis-seeding subclones before relapse.
Trial registration: ClinicalTrials.gov NCT01888601.
© 2023. The Author(s).
Conflict of interest statement
M.A.B. has consulted for Achilles Therapeutics. D.A.M. reports speaker fees from AstraZeneca, Eli Lilly and Takeda, consultancy fees from AstraZeneca, Thermo Fisher Scientific, Takeda, Amgen, Janssen, MIM Software, Bristol Myers Squibb (BMS) and Eli Lilly and has received educational support from Takeda and Amgen. S.V. is listed as a co-inventor on a patent for detecting molecules in a sample (U.S. patent no. 10578620). A.M.F. is listed as a co-inventor on a patent application to determine methods and systems for tumour monitoring (PCT/EP2022/077987). C.A. has received speaking honoraria or expenses from Novartis, Roche, AstraZeneca and BMS and reports employment at AstraZeneca; is listed as an inventor on a European patent application relating to assay technology to detect tumour recurrence (PCT/GB2017/053289), the patent has been licensed to commercial entities and, under his terms of employment, C.A is due a revenue share of any revenue generated from such license(s); declares a patent application (PCT/US2017/028013) for methods to detect lung cancer; and is a named inventor on a patent application to determine methods and systems for tumour monitoring (PCT/EP2022/077987); and is a named inventor on a provisional patent protection related to a ctDNA detection algorithm. C.T.H. has received speaker fees from AstraZeneca. G.A.W. is employed by and has stock options in Achilles Therapeutics. R.S. reports non-financial support from Merck and BMS, research support from Merck, Puma Biotechnology and Roche, and personal fees from Roche, BMS and Exact Sciences for advisory boards. D.A.F reports grants from Aldeyra, Boehringer Ingelheim, Astex Therapeutics, Bayer, BMS, GSK, RS Oncology, Clovis, Eli Lilly, BMS, MSD and GSK, and personal fees from Atara, BMS, Boehringer Ingelheim, Cambridge Clinical Laboratories, Targovax, Roche and RS Oncology. C.R.L. has provided consulting/advisory support to Amgen and Hanson Wade, and educational support to Amgen; and has received financial support for research from Revolution Medicines, as well as non-financial support from Amgen. J.C. reports funding from Amgen to attend a conference. A.N. reports personal fees from Aidence BV and Faculty Science Limited. N.N. reports honoraria for non-promotional educational talks, advisory boards or conference attendance from Amgen, AstraZeneca, Boehringer Ingelheim, BMS, Fujifilm, Guardant Health, Intuitive, Janssen, Lilly, Merck Sharp & Dohme, Olympus, OncLive, PeerVoice, Pfizer and Takeda. S.M.J. has received fees for advisory board membership in the last three years from Astra-Zeneca, Bard1 Lifescience and Johnson and Johnson, grant income from Owlstone and GRAIL, and assistance with travel to an academic meeting from Cheisi. M.D.F. acknowledges grant support from CRUK, AstraZeneca, Boehringer Ingelheim, MSD and Merck; is an advisory board member for Transgene; and has consulted for Achilles, Amgen, AstraZeneca, Bayer, Boxer, BMS, Celgene, EQRx, Guardant Health, Immutep, Ixogen, Janssen, Merck, MSD, Nanobiotix, Novartis, Oxford VacMedix, Pharmamar, Pfizer, Roche, Takeda and UltraHuman. S.A.Q. is a co-founder, stockholder and chief scientific officer of Achilles Therapeutics. K.S.P is a co-founder of Achilles Therapeutics. C.D. received research funding/educational research grants from AstraZeneca, Astex Pharmaceuticals, Bioven, Amgen, Carrick Therapeutics, Merck, Taiho Oncology, GSK, Bayer, Boehringer Ingelheim, Roche, BMS, Novartis, Celgene, Epigene Therapeutics, Angle, Menarini, Clearbridge Biomedics, Thermo Fisher Scientific and Neomed Therapeutics; and received honoraria for consultancy and/or advisory boards from Biocartis, Merck, AstraZeneca, GRAIL and Boehringer Ingelheim. A.Ha. has received fees for being a member of independent data monitoring committees for Roche-sponsored clinical trials, and academic projects co-ordinated by Roche. N.J.B. is listed as a co-inventor on a patent to identify responders to cancer treatment (PCT/GB2018/051912) and a co-inventor on a patent for methods for predicting anti-cancer response (US14/466,208). M.J.-H. has consulted for, and is a member of, the Achilles Therapeutics scientific advisory board and steering committee, has received speaker honoraria from Pfizer, Astex Pharmaceuticals and Oslo Cancer Cluster, and is listed as a co-inventor on a European patent application relating to methods to detect lung cancer PCT/US2017/028013); this patent has been licensed to commercial entities and, under terms of employment, M.J.-H. is due a share of any revenue generated from such license(s). N.M. has received consultancy fees and has stock options in Achilles Therapeutics; and holds European patents relating to targeting neoantigens (PCT/EP2016/059401), identifying patient response to immune checkpoint blockade (PCT/EP2016/071471), determining HLA LOH (PCT/GB2018/052004), and predicting survival rates of patients with cancer (PCT/GB2020/050221). C.S. acknowledges grant support from AstraZeneca, Boehringer-Ingelheim, BMS, Pfizer, Roche-Ventana, Invitae (previously Archer Dx, collaboration in minimal residual disease sequencing technologies), Ono Pharmaceutical, and Personalis; is an AstraZeneca advisory board member and chief investigator for the AZ MeRmaiD 1 and 2 clinical trials and is also co-chief investigator of the NHS Galleri trial funded by GRAIL and a paid member of GRAIL’s scientific advisory board; receives consultant fees from Achilles Therapeutics (also a scientific advisory board member), Bicycle Therapeutics (also a scientific advisory board member), Genentech, Medicxi, China Innovation Centre of Roche (CICoR) formerly Roche Innovation Centre – Shanghai, Metabomed (until July 2022) and the Sarah Cannon Research Institute; has received honoraria from Amgen, AstraZeneca, Pfizer, Novartis, GlaxoSmithKline, MSD, Bristol Myers Squibb, Illumina, and Roche-Ventana; had stock options in Apogen Biotechnologies and GRAIL until June 2021, and currently has stock options in Epic Bioscience, Bicycle Therapeutics, and has stock options and is co-founder of Achilles Therapeutics; is listed as an inventor on a European patent application relating to assay technology to detect tumour recurrence (PCT/GB2017/053289), the patent has been licensed to commercial entities and, under his terms of employment, C.S. is due a revenue share of any revenue generated from such license(s); holds patents relating to targeting neoantigens (PCT/EP2016/059401), identifying patient response to immune checkpoint blockade (PCT/EP2016/071471), determining HLA LOH (PCT/GB2018/052004), predicting survival rates of patients with cancer (PCT/GB2020/050221), identifying patients who respond to cancer treatment (PCT/GB2018/051912), a US patent relating to detecting tumour mutations (PCT/US2017/28013), methods for lung cancer detection (US20190106751A1) and both a European and US patent related to identifying insertion/deletion mutation targets (PCT/GB2018/051892) and is listed as a co-inventor on a patent application to determine methods and systems for tumour monitoring (PCT/EP2022/077987) and is a named inventor on a provisional patent protection related to a ctDNA detection algorithm.
Figures
Comment in
-
Molecular portraits of lung cancer evolution.Nature. 2023 Apr;616(7957):435-436. doi: 10.1038/d41586-023-00934-0. Nature. 2023. PMID: 37045956 No abstract available.
References
-
- Grigoriadis, K. et al. CONIPHER: a computational framework for scalable phylogenetic reconstruction with error correction. Protoc. Exchange10.21203/rs.3.pex-2158/v1 (2023). - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- CTRNBC-2022/100001/CRUK_/Cancer Research UK/United Kingdom
- 25354/CRUK_/Cancer Research UK/United Kingdom
- 30025/CRUK_/Cancer Research UK/United Kingdom
- CC2041/WT_/Wellcome Trust/United Kingdom
- MR/V033077/1/MRC_/Medical Research Council/United Kingdom
- MR/T02481X/1/MRC_/Medical Research Council/United Kingdom
- 29569/CRUK_/Cancer Research UK/United Kingdom
- MR/W025051/1/MRC_/Medical Research Council/United Kingdom
- 21999/CRUK_/Cancer Research UK/United Kingdom
- 24956/CRUK_/Cancer Research UK/United Kingdom
- CC2008/WT_/Wellcome Trust/United Kingdom
- 25349/CRUK_/Cancer Research UK/United Kingdom
- 17786/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
