

Propofol and survival: an updated meta-analysis of randomized clinical trials
- PMID: 37046269
- PMCID: PMC10099692
- DOI: 10.1186/s13054-023-04431-8
Propofol and survival: an updated meta-analysis of randomized clinical trials
Abstract
Background: Propofol is one of the most widely used hypnotic agents in the world. Nonetheless, propofol might have detrimental effects on clinically relevant outcomes, possibly due to inhibition of other interventions' organ protective properties. We performed a systematic review and meta-analysis of randomized controlled trials to evaluate if propofol reduced survival compared to any other hypnotic agent in any clinical setting.
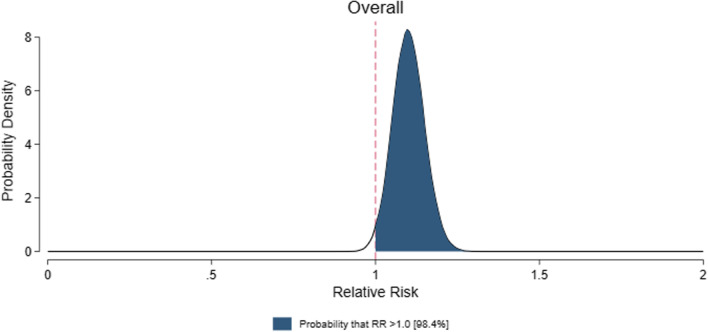
Methods: We searched eligible studies in PubMed, Google Scholar, and the Cochrane Register of Clinical Trials. The following inclusion criteria were used: random treatment allocation and comparison between propofol and any comparator in any clinical setting. The primary outcome was mortality at the longest follow-up available. We conducted a fixed-effects meta-analysis for the risk ratio (RR). Using this RR and 95% confidence interval, we estimated the probability of any harm (RR > 1) through Bayesian statistics. We registered this systematic review and meta-analysis in PROSPERO International Prospective Register of Systematic Reviews (CRD42022323143).
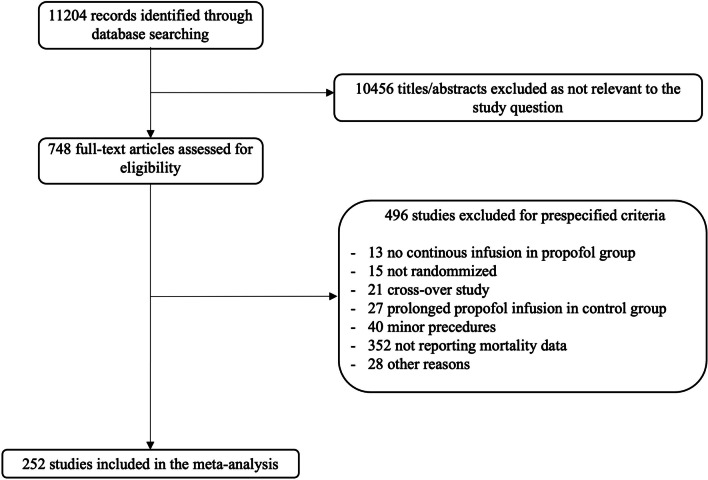
Results: We identified 252 randomized trials comprising 30,757 patients. Mortality was higher in the propofol group than in the comparator group (760/14,754 [5.2%] vs. 682/16,003 [4.3%]; RR = 1.10; 95% confidence interval, 1.01-1.20; p = 0.03; I2 = 0%; number needed to harm = 235), corresponding to a 98.4% probability of any increase in mortality. A statistically significant mortality increase in the propofol group was confirmed in subgroups of cardiac surgery, adult patients, volatile agent as comparator, large studies, and studies with low mortality in the comparator arm.
Conclusions: Propofol may reduce survival in perioperative and critically ill patients. This needs careful assessment of the risk versus benefit of propofol compared to other agents while planning for large, pragmatic multicentric randomized controlled trials to provide a definitive answer.
Keywords: Anesthesia; Hypnotics; Meta-analysis; Mortality; Organ protection; Propofol; Systematic review; Volatile anesthetics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Clinical Frailty Scale and the FRAIL checklist: Can they complement each other?Crit Care. 2023 May 4;27(1):171. doi: 10.1186/s13054-023-04451-4. Crit Care. 2023. PMID: 37143077 Free PMC article. No abstract available.
-
Reply to "Propofol and survival: an updated meta‑analysis of randomized clinical trials".Crit Care. 2023 May 17;27(1):192. doi: 10.1186/s13054-023-04484-9. Crit Care. 2023. PMID: 37198651 Free PMC article. No abstract available.
-
Comment to: Propofol and survival: an updated meta-analysis of randomized clinical trials.Crit Care. 2023 May 24;27(1):198. doi: 10.1186/s13054-023-04489-4. Crit Care. 2023. PMID: 37226253 Free PMC article. No abstract available.
-
Propofol versus the world: The whole is not always greater than the sum of its parts.Crit Care. 2023 May 30;27(1):208. doi: 10.1186/s13054-023-04450-5. Crit Care. 2023. PMID: 37254187 Free PMC article. No abstract available.
-
Comment to: "Propofol and survival: an updated meta-analysis of randomized clinical trials": authors' reply.Crit Care. 2023 Jun 15;27(1):237. doi: 10.1186/s13054-023-04528-0. Crit Care. 2023. PMID: 37322553 Free PMC article. No abstract available.
-
Authors' reply to the comment from Benavides-Zora et al.Crit Care. 2023 Jun 29;27(1):255. doi: 10.1186/s13054-023-04547-x. Crit Care. 2023. PMID: 37386506 Free PMC article. No abstract available.
-
Harmful effects of propofol? The Editor's standpoint.Crit Care. 2023 Jul 10;27(1):279. doi: 10.1186/s13054-023-04559-7. Crit Care. 2023. PMID: 37430324 Free PMC article. No abstract available.
-
Comment on Propofol and survival: an updated meta-analysis of randomized clinical trials.Crit Care. 2023 Jul 11;27(1):281. doi: 10.1186/s13054-023-04550-2. Crit Care. 2023. PMID: 37434188 Free PMC article. No abstract available.
-
Propofol curtails survival in perioperative and critically ill patients by a relative reduction of 10%: should propofol be abandoned?Ann Transl Med. 2024 Oct 20;12(5):98. doi: 10.21037/atm-24-52. Epub 2024 Aug 30. Ann Transl Med. 2024. PMID: 39507444 Free PMC article. No abstract available.
Similar articles
-
Propofol and survival: a meta-analysis of randomized clinical trials.Acta Anaesthesiol Scand. 2015 Jan;59(1):17-24. doi: 10.1111/aas.12415. Epub 2014 Oct 14. Acta Anaesthesiol Scand. 2015. PMID: 25312519
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Safety and Efficacy of the Combination of Propofol and Ketamine for Procedural Sedation/Anesthesia in the Pediatric Population: A Systematic Review and Meta-analysis.Anesth Analg. 2021 Apr 1;132(4):979-992. doi: 10.1213/ANE.0000000000004967. Anesth Analg. 2021. PMID: 32665470
-
Hypnotic agents for induction of general anesthesia in cesarean section patients: A systematic review and meta-analysis of randomized controlled trials.J Clin Anesth. 2018 Aug;48:73-80. doi: 10.1016/j.jclinane.2018.04.010. Epub 2018 May 26. J Clin Anesth. 2018. PMID: 29778972
-
Comparison of the recovery quality between remimazolam and propofol after general anesthesia: systematic review and a meta-analysis of randomized controlled trials.PeerJ. 2024 Aug 26;12:e17930. doi: 10.7717/peerj.17930. eCollection 2024. PeerJ. 2024. PMID: 39210920 Free PMC article.
Cited by
-
The effects of ciprofol on haemodynamics under general anaesthesia during thoracoscopic surgery: a randomised, double-blind, controlled trial.BMC Anesthesiol. 2025 Apr 10;25(1):168. doi: 10.1186/s12871-025-03054-6. BMC Anesthesiol. 2025. PMID: 40211149 Free PMC article. Clinical Trial.
-
2024 EACTS/EACTAIC/EBCP Guidelines on cardiopulmonary bypass in adult cardiac surgery.Br J Anaesth. 2025 Apr;134(4):917-1008. doi: 10.1016/j.bja.2025.01.015. Epub 2025 Feb 14. Br J Anaesth. 2025. PMID: 39955230 Free PMC article.
-
[Focus on sepsis and general intensive care medicine : Summary of selected intensive care studies].Anaesthesiologie. 2023 Nov;72(11):821-830. doi: 10.1007/s00101-023-01334-9. Epub 2023 Sep 6. Anaesthesiologie. 2023. PMID: 37672061 German. No abstract available.
-
Harmful effects of propofol? The Editor's standpoint.Crit Care. 2023 Jul 10;27(1):279. doi: 10.1186/s13054-023-04559-7. Crit Care. 2023. PMID: 37430324 Free PMC article. No abstract available.
-
Reply to "Propofol and survival: an updated meta‑analysis of randomized clinical trials".Crit Care. 2023 May 17;27(1):192. doi: 10.1186/s13054-023-04484-9. Crit Care. 2023. PMID: 37198651 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
