

Metastasis pattern and prognosis in children with neuroblastoma
- PMID: 37046344
- PMCID: PMC10091559
- DOI: 10.1186/s12957-023-03011-y
Metastasis pattern and prognosis in children with neuroblastoma
Abstract
Background: We aimed to investigate the different metastases and prognoses of neuroblastoma (NB) and determine the risk factors of metastasis.
Method: Data of 1224 patients with NB were obtained from the Surveillance, Epidemiology and End Results database (2010-2018). Pearson's chi-square test, Kaplan-Meier analysis, multivariable logistic regression and Cox regression analysis were used to determine the factors associated with prognosis.
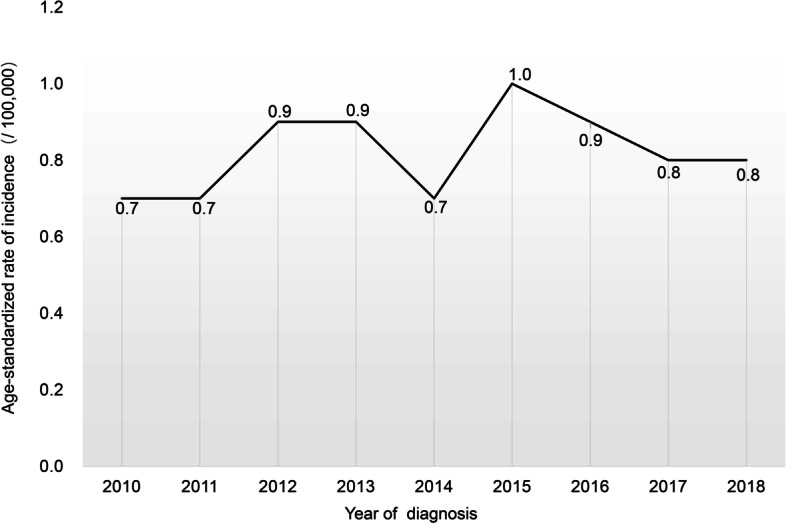
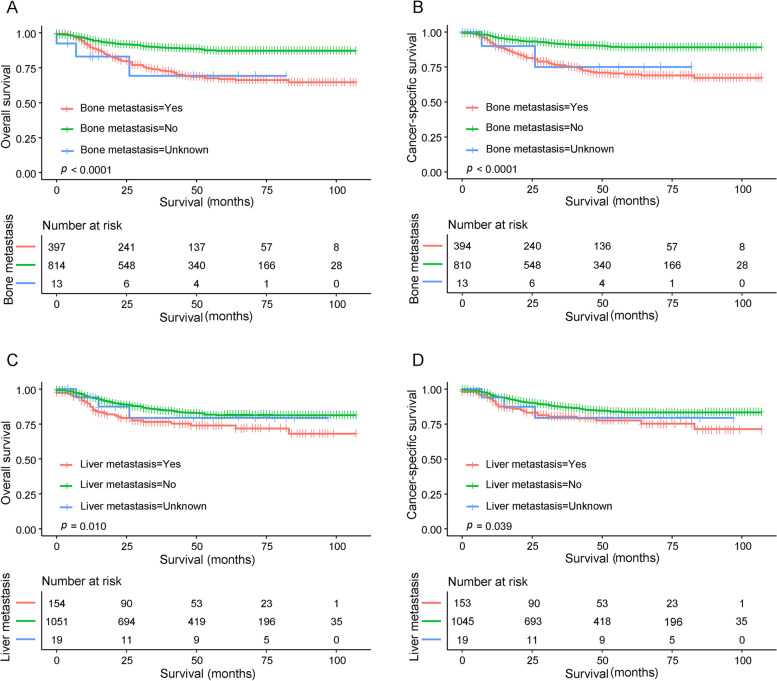
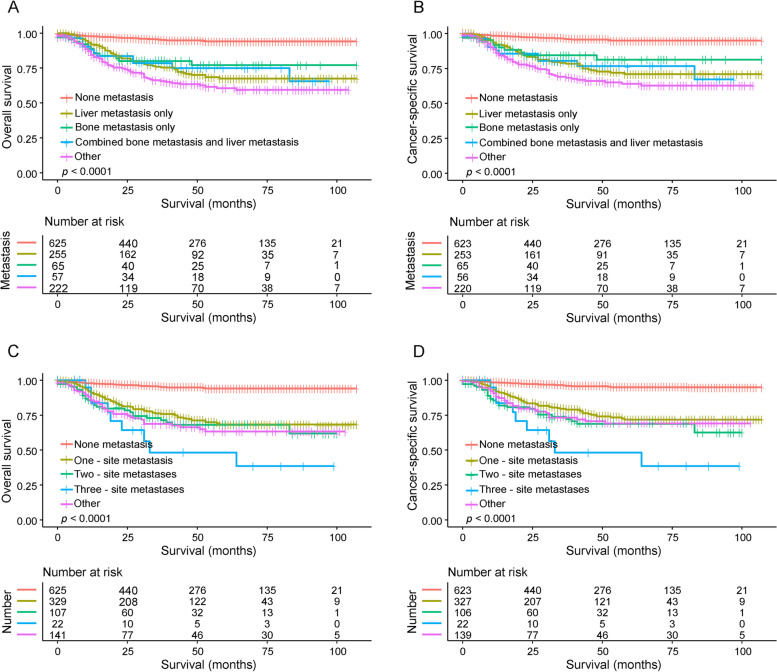
Results: The overall incidence of NB was an age-adjusted rate of 8.2 patients per 1,000,000 children. In total, 1224 patients were included in our study, with 599 patients (48.9%) exhibiting distant metastases. Compared to patients with non-metastatic NB, a greater proportion of patients with metastatic NB were under 1 year, male, had an adrenal primary site, unilateral tumour, a tumour size > 10 cm, neuroblastoma-not otherwise specified (NB-NOS), second malignant neoplasms and were more likely to choose radiotherapy and chemotherapy. Multivariate Cox regression showed that metastasis was an independent risk factor for overall survival (OS) and cancer-specific survival (CSS). The survival rate of non-metastatic patients with NB was better than those with metastasis (OS: hazard ratio (HR): 0.248, P < 0.001; CSS: HR: 0.267, P < 0.001). The bone and liver were the two most common isolated metastatic sites in NB. However, no statistical difference was observed in OS and CSS between the only bone metastasis group, only liver metastasis group and bone metastasis combined with liver metastasis group (all P > 0.05). Additionally, age at diagnosis > 1 year (odds ratio (OR): 3.295, P < 0 .001), grades III-IV (OR: 26.228, P < 0 .001) and 5-10 cm tumours (OR: 1.781, P < 0 .001) increased the risk of bone metastasis of NB. Moreover, no surgical treatment (OR: 2.441, P < 0 .001) increased the risk of liver metastasis of NB.
Conclusion: Metastatic NB has unique clinicopathological features, with the bone and liver as the most common single metastatic sites of NB. Therefore, more aggressive treatment is recommended for high-risk children with NB displaying distant metastases.
Keywords: Cancer-specific survival; Distant metastases; Neuroblastoma; Overall survival; SEER.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- London WB, Bagatell R, Weigel BJ, et al. Historical time to disease progression and progression-free survival in patients with recurrent/refractory neuroblastoma treated in the modern era on Children’s Oncology Group early-phase trials. Cancer. 2017;123(24):4914–4923. doi: 10.1002/cncr.30934. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
