

Continuous glucose monitoring in patients with post-bariatric hypoglycaemia reduces hypoglycaemia and glycaemic variability
- PMID: 37046360
- PMCID: PMC10807851
- DOI: 10.1111/dom.15096
Continuous glucose monitoring in patients with post-bariatric hypoglycaemia reduces hypoglycaemia and glycaemic variability
Abstract
Aim: To determine whether continuous glucose monitoring (CGM) can reduce hypoglycaemia in patients with post-bariatric hypoglycaemia (PBH).
Materials and methods: In an open-label, nonrandomized, pre-post design with sequential assignment, CGM data were collected in 22 individuals with PBH in two sequential phases: (i) masked (no access to sensor glucose or alarms); and (ii) unmasked (access to sensor glucose and alarms for low or rapidly declining sensor glucose). Twelve participants wore the Dexcom G4 device for a total of 28 days, while 10 wore the Dexcom G6 device for a total of 20 days.
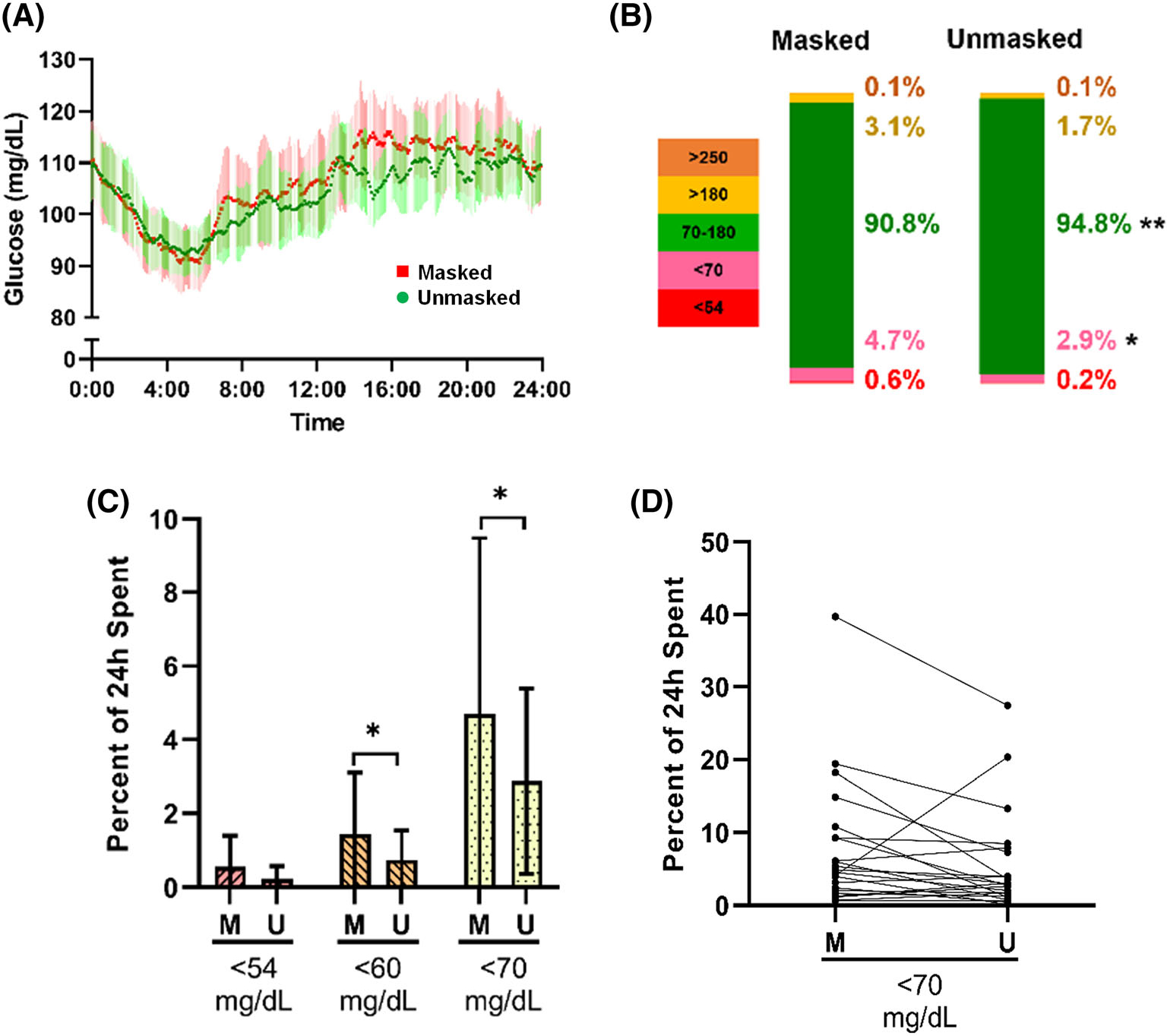
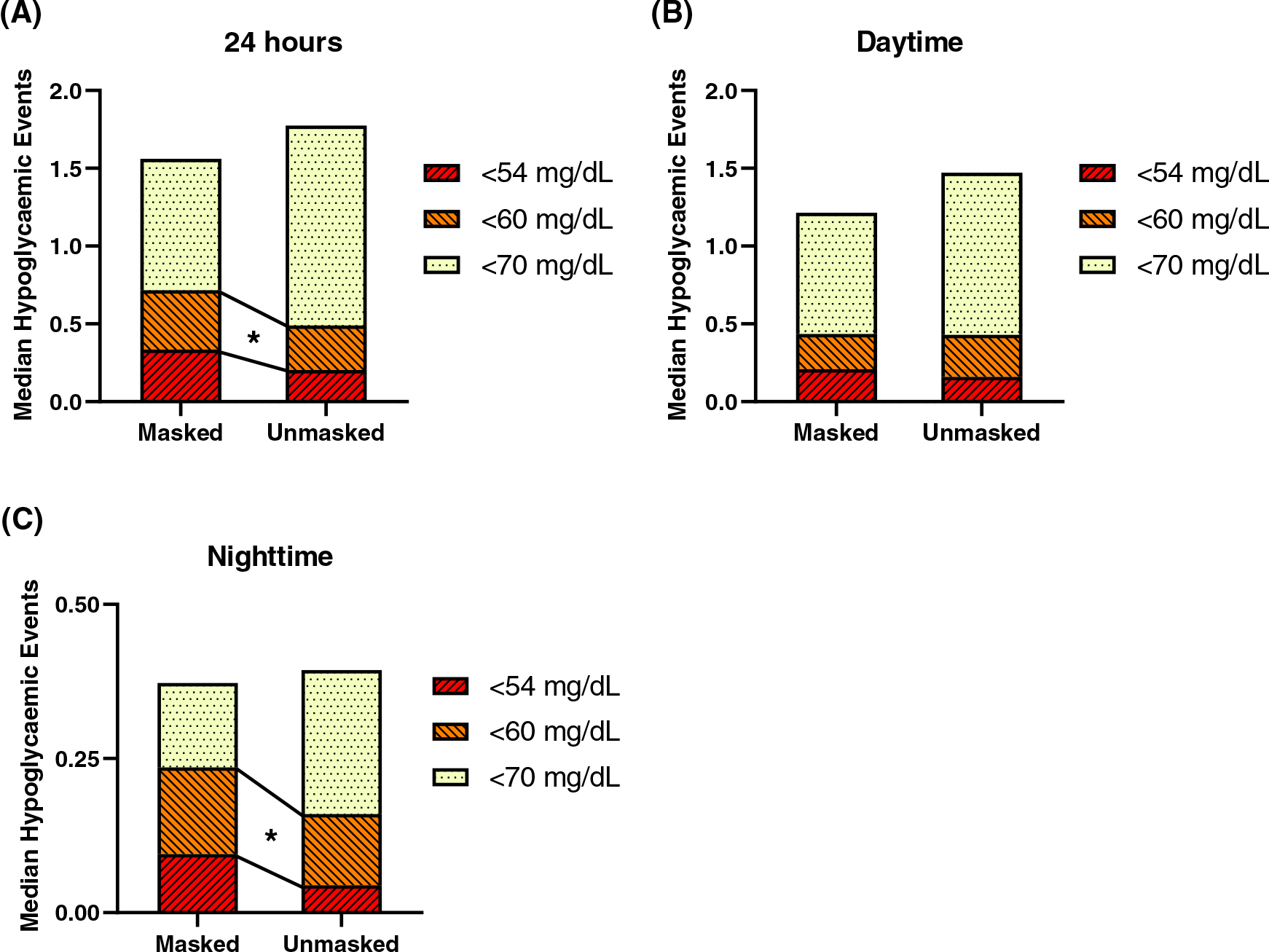
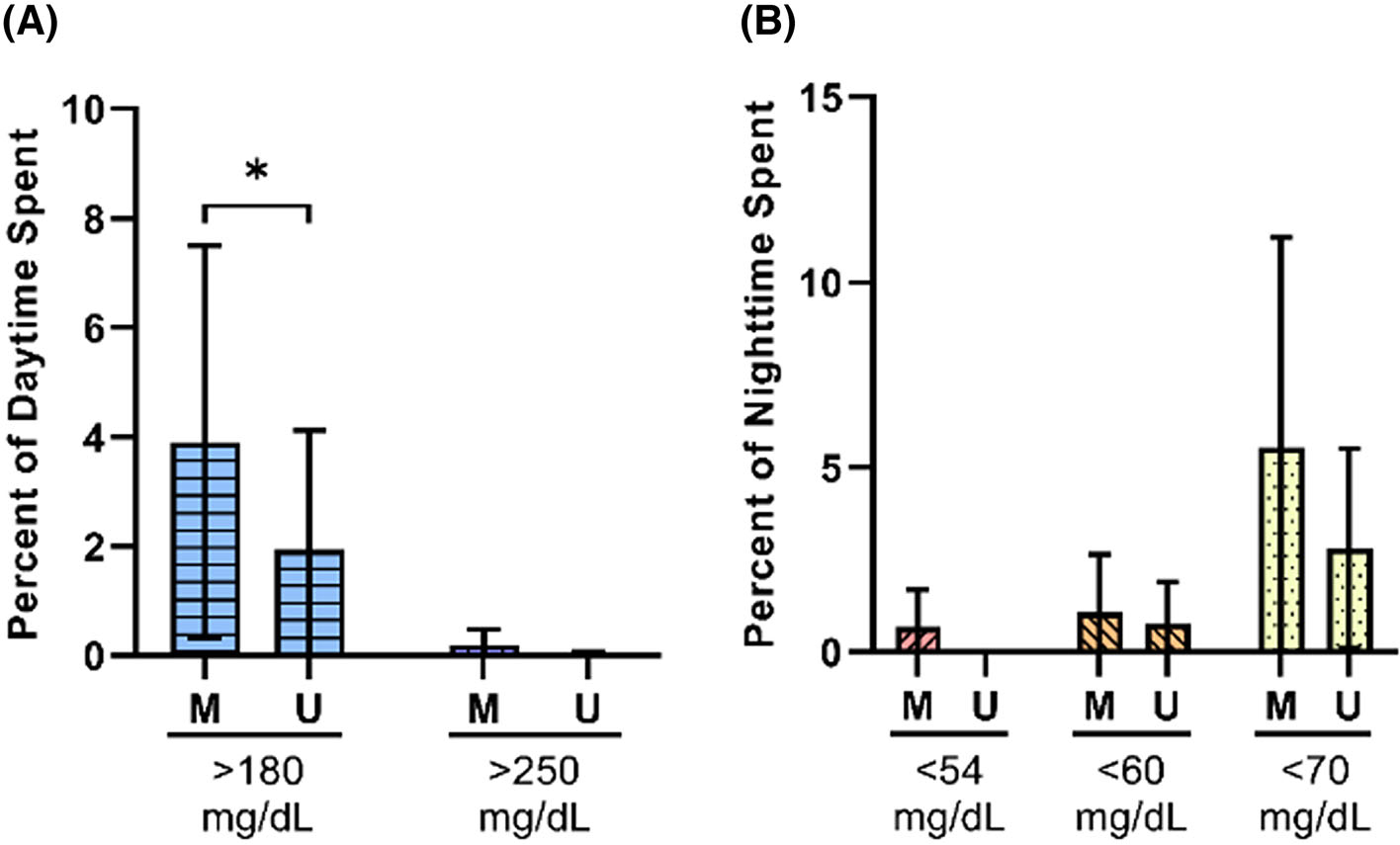
Results: Participants with PBH spent a lower percentage of time in hypoglycaemia over 24 hours with unmasked versus masked CGM (<3.3 mM/L, or <60 mg/dL: median [median absolute deviation {MAD}] 0.7 [0.8]% vs. 1.4 [1.7]%, P = 0.03; <3.9 mM/L, or <70 mg/dL: median [MAD] 2.9 [2.5]% vs. 4.7 [4.8]%; P = 0.04), with similar trends overnight. Sensor glucose data from the unmasked phase showed a greater percentage of time spent between 3.9 and 10 mM/L (70-180 mg/dL) (median [MAD] 94.8 [3.9]% vs. 90.8 [5.2]%; P = 0.004) and lower glycaemic variability over 24 hours (median [MAD] mean amplitude of glycaemic excursion 4.1 [0.98] vs. 4.4 [0.99] mM/L; P = 0.04). During the day, participants also spent a greater percentage of time in normoglycaemia with unmasked CGM (median [MAD] 94.2 [4.8]% vs. 90.9 [6.2]%; P = 0.005), largely due to a reduction in hyperglycaemia (>10 mM/L, or 180 mg/dL: median [MAD] 1.9 [2.2]% vs. 3.9 [3.6]%; P = 0.02).
Conclusions: Real-time CGM data and alarms are associated with reductions in low sensor glucose, elevated sensor glucose, and glycaemic variability. This suggests CGM allows patients to detect hyperglycaemic peaks and imminent hypoglycaemia, allowing dietary modification and self-treatment to reduce hypoglycaemia. The use of CGM devices may improve safety in PBH, particularly for patients with hypoglycaemia unawareness.
Keywords: bariatric surgery; continuous glucose monitoring; glycaemic control; hypoglycaemia.
© 2023 John Wiley & Sons Ltd.
Conflict of interest statement
DISCLOSURE OF INTERESTS
Funding for this study was received via an investigator-initiated research grant to Mary Elizabeth Patti from Dexcom. Data analysis and manuscript preparation were performed by the study team without input from Dexcom. We also acknowledge support from the Diabetes Research Center grant P30 DK 036836. Mary Elizabeth Patti reports personal consulting fees from Astra Zeneca, Fractyl, Hanmi Pharmaceutical, MBX Biosciences, Recordati, Poxel, and Eiger Pharmaceuticals and grants from the Chan-Zuckerberg Initiative and Helmsley Trust, outside the submitted work. Donald C. Simonson is a stockholder/shareholder of GI Windows and his spouse is owner of Phase V Technologies (neither related to the current study).
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
