

Pathomorphological Diagnostic Criteria for Focal Cortical Dysplasias and Other Common Epileptogenic Lesions-Review of the Literature
- PMID: 37046529
- PMCID: PMC10092959
- DOI: 10.3390/diagnostics13071311
Pathomorphological Diagnostic Criteria for Focal Cortical Dysplasias and Other Common Epileptogenic Lesions-Review of the Literature
Abstract
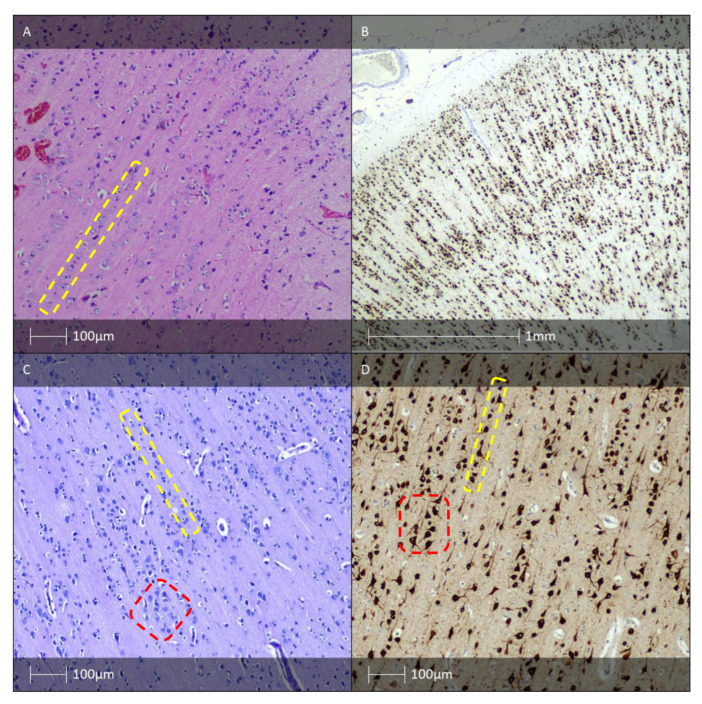
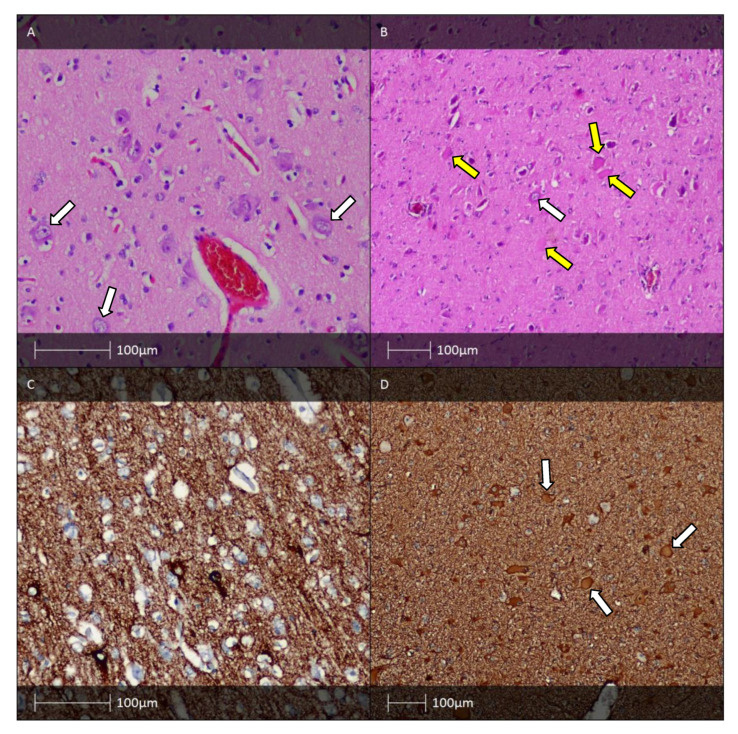
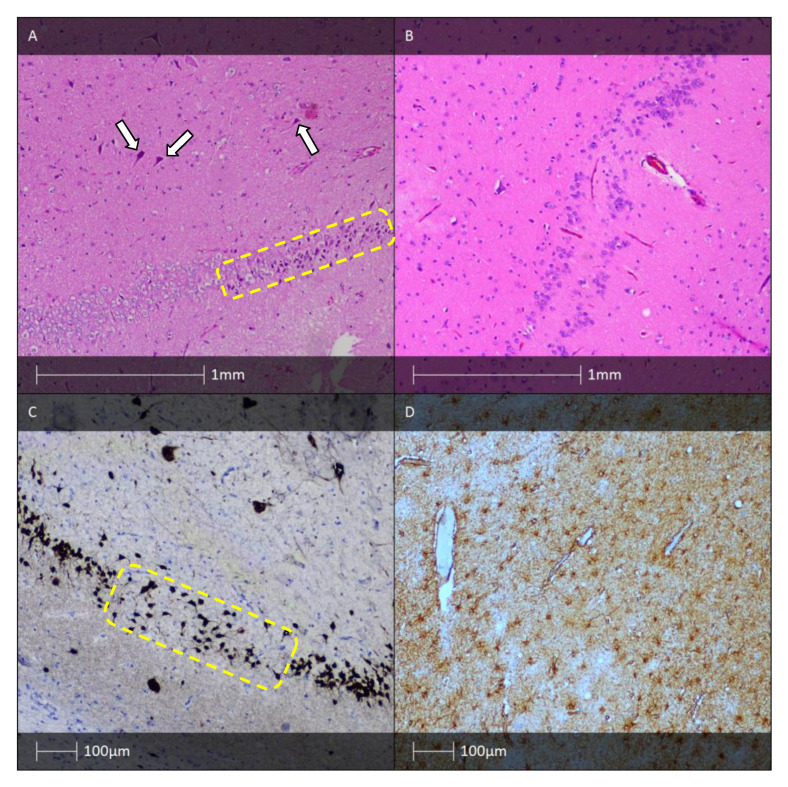
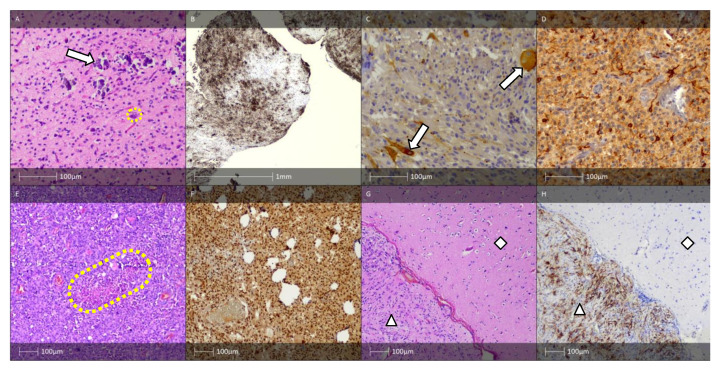
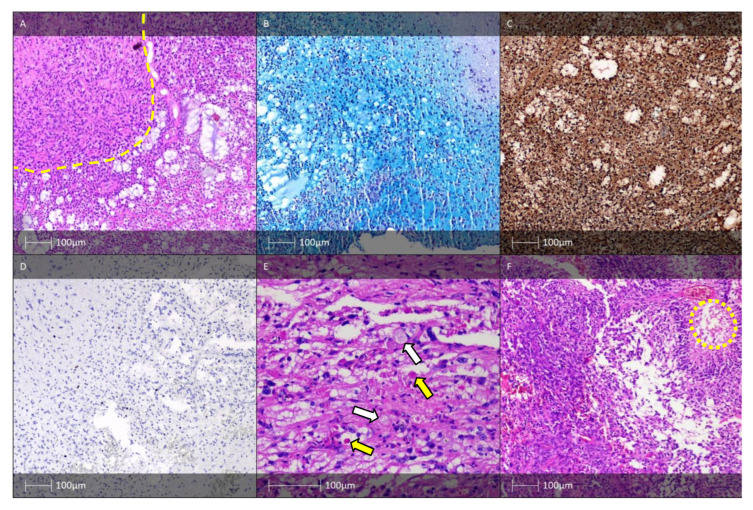
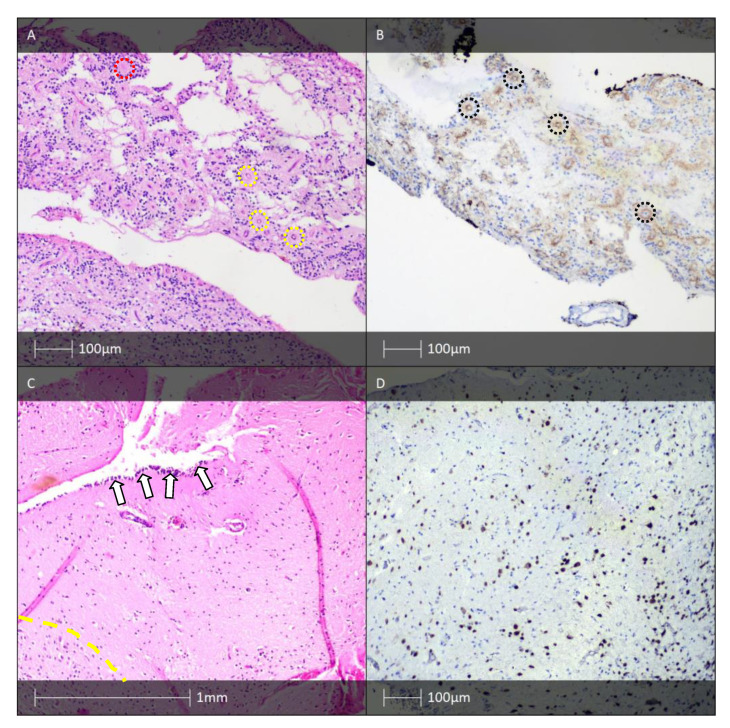
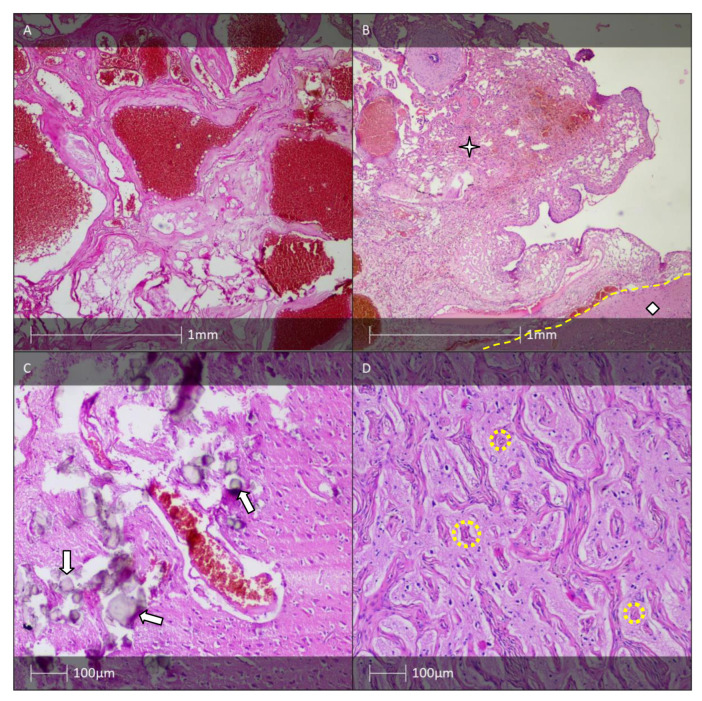
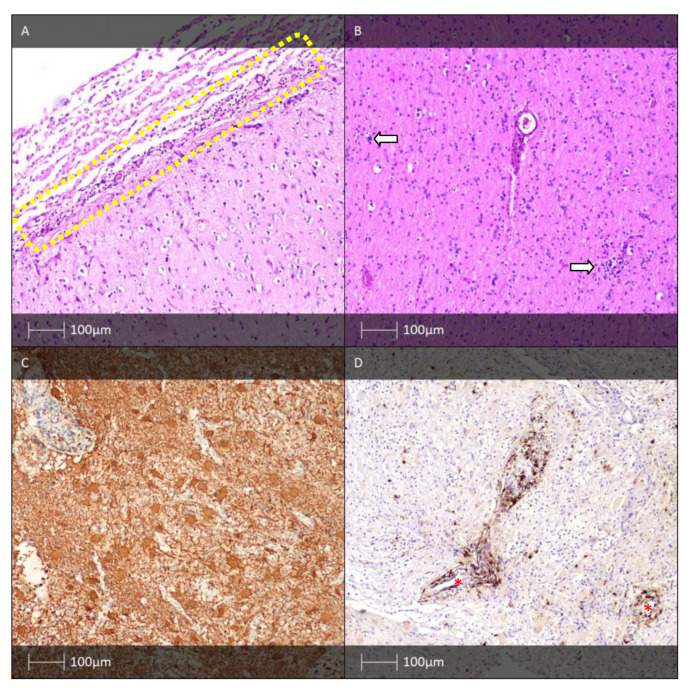
Focal cortical dysplasia (FCD) represents a heterogeneous group of morphological changes in the brain tissue that can predispose the development of pharmacoresistant epilepsy (recurring, unprovoked seizures which cannot be managed with medications). This group of neurological disorders affects not only the cerebral cortex but also the subjacent white matter. This work reviews the literature describing the morphological substrate of pharmacoresistant epilepsy. All illustrations presented in this study are obtained from brain biopsies from refractory epilepsy patients investigated by the authors. Regarding classification, there are three main FCD types, all of which involve cortical dyslamination. The 2022 revision of the International League Against Epilepsy (ILAE) FCD classification includes new histologically defined pathological entities: mild malformation of cortical development (mMCD), mild malformation of cortical development with oligodendroglial hyperplasia in frontal lobe epilepsy (MOGHE), and "no FCD on histopathology". Although the pathomorphological characteristics of the various forms of focal cortical dysplasias are well known, their aetiologic and pathogenetic features remain elusive. The identification of genetic variants in FCD opens an avenue for novel treatment strategies, which are of particular utility in cases where total resection of the epileptogenic area is impossible.
Keywords: focal cortical dysplasia; mild malformation of cortical development; pharmacoresistant epilepsy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The ILAE consensus classification of focal cortical dysplasia: An update proposed by an ad hoc task force of the ILAE diagnostic methods commission.Epilepsia. 2022 Aug;63(8):1899-1919. doi: 10.1111/epi.17301. Epub 2022 Jun 15. Epilepsia. 2022. PMID: 35706131 Free PMC article.
-
Mild malformation of cortical development with oligodendroglial hyperplasia and epilepsy (MOGHE): a widespread disease with an apparently focal epilepsy.Epileptic Disord. 2021 Apr 1;23(2):407-411. doi: 10.1684/epd.2021.1280. Epileptic Disord. 2021. PMID: 33935026
-
Neuropathological work-up of focal cortical dysplasias using the new ILAE consensus classification system - practical guideline article invited by the Euro-CNS Research Committee.Clin Neuropathol. 2011 Jul-Aug;30(4):164-77. doi: 10.5414/np300398. Clin Neuropathol. 2011. PMID: 21726501
-
SLC35A2 somatic variants in drug resistant epilepsy: FCD and MOGHE.Neurobiol Dis. 2023 Oct 15;187:106299. doi: 10.1016/j.nbd.2023.106299. Epub 2023 Sep 20. Neurobiol Dis. 2023. PMID: 37739137 Free PMC article. Review.
-
Variable histopathology features of neuronal dyslamination in the cerebral neocortex adjacent to epilepsy-associated vascular malformations suggest complex pathogenesis of focal cortical dysplasia ILAE type IIIc.Brain Pathol. 2022 Sep;32(5):e13052. doi: 10.1111/bpa.13052. Epub 2022 Jan 9. Brain Pathol. 2022. PMID: 35001442 Free PMC article. Review.
Cited by
-
Bridging Development and Disruption: Comprehensive Insights into Focal Cortical Dysplasia and Epileptic Management.Cureus. 2023 Sep 26;15(9):e45996. doi: 10.7759/cureus.45996. eCollection 2023 Sep. Cureus. 2023. PMID: 37900524 Free PMC article. Review.
-
The role of genetic testing in evaluating surgical outcomes for pediatric focal cortical dysplasia associated with NPRL3 variant.Epilepsy Behav Rep. 2025 Jul 16;32:100808. doi: 10.1016/j.ebr.2025.100808. eCollection 2025 Dec. Epilepsy Behav Rep. 2025. PMID: 40718049 Free PMC article.
-
WONOEP appraisal: The role of glial cells in focal malformations associated with early onset epilepsies.Epilepsia. 2024 Dec;65(12):3457-3468. doi: 10.1111/epi.18126. Epub 2024 Oct 14. Epilepsia. 2024. PMID: 39401070 Free PMC article. Review.
References
-
- Milanov I., Bozhinova V. National Consensus on the Diagnosis and Treatment of Epilepsy. Bulgarian Society of Neurology; Golden Sands, Bulgaria: 2022. p. 6.
-
- Kwan P., Arzimanoglou A., Berg A.T., Brodie M.J., Hauser W.A., Mathern G., Moshé S.L., Perucca E., Wiebe S., French J. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51:1069–1077. doi: 10.1111/j.1528-1167.2009.02397.x. - DOI - PubMed
-
- Minkin K. Ph.D. Thesis. Medical University-Sofia; Sofia, Bulgaria: 2009. Surgical Treatment Options for Patients with Symptomatic Pharmacoresistant Epilepsy.
-
- Najm I., Lal D., Alonso Vanegas M., Cendes F., Lopes-Cendes I., Palmini A., Paglioli E., Sarnat H.B., Walsh C.A., Wiebe S., et al. The ILAE consensus classification of Focal Cortical Dysplasia (FCD): An update proposed by a hoc Task Force of ILAE Diagnostic Methods commission. Epilepsia. 2022;63:1899–1919. doi: 10.1111/epi.17301. - DOI - PMC - PubMed
-
- Schurr J., Coras R., Rössler K., Pieper T., Kudernatsch M., Holthausen H., Winkler P., Woermann F., Bien C.G., Polster T., et al. Mild malformation of cortical development with oligodendroglial hyperplasia in frontal lobe epilepsy: A new clinic-pathological entity. Brain Pathol. 2017;27:26–35. doi: 10.1111/bpa.12347. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
