

Effectiveness of Colorectal Cancer (CRC) Screening on All-Cause and CRC-Specific Mortality Reduction: A Systematic Review and Meta-Analysis
- PMID: 37046609
- PMCID: PMC10093633
- DOI: 10.3390/cancers15071948
Effectiveness of Colorectal Cancer (CRC) Screening on All-Cause and CRC-Specific Mortality Reduction: A Systematic Review and Meta-Analysis
Abstract
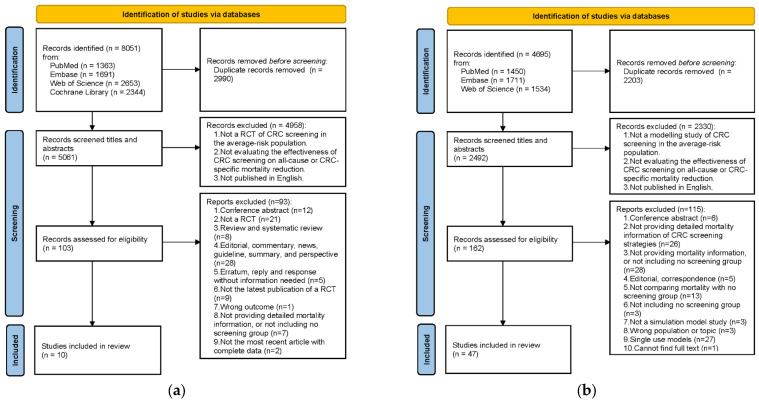
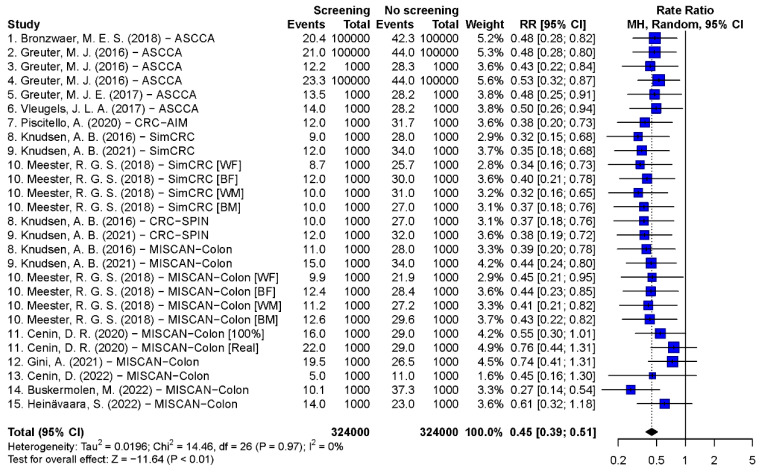
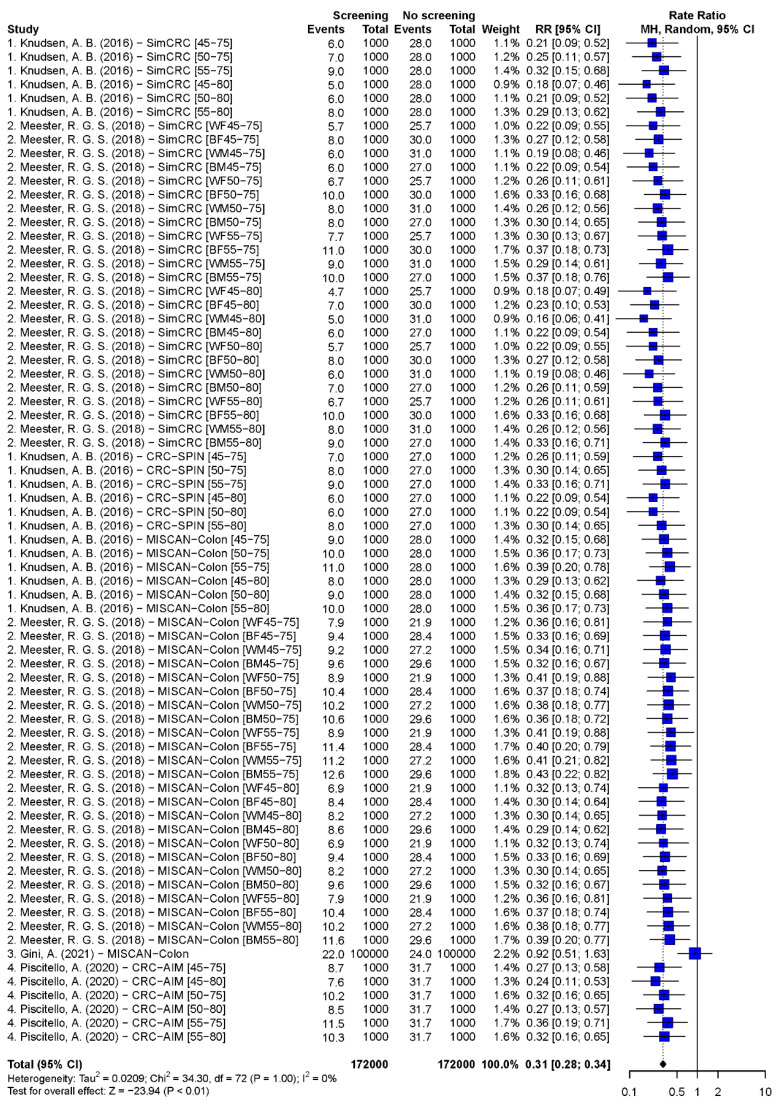
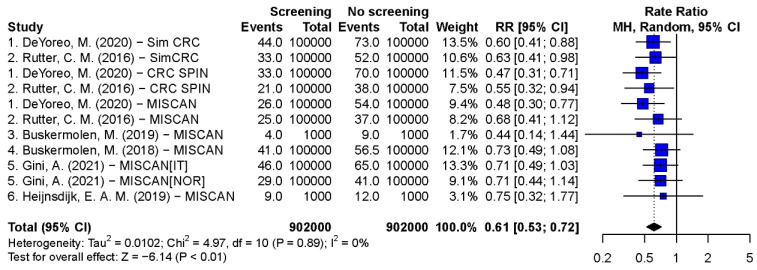
(1) Background: The aim of this study was to pool and compare all-cause and colorectal cancer (CRC) specific mortality reduction of CRC screening in randomized control trials (RCTs) and simulation models, and to determine factors that influence screening effectiveness. (2) Methods: PubMed, Embase, Web of Science and Cochrane library were searched for eligible studies. Multi-use simulation models or RCTs that compared the mortality of CRC screening with no screening in general population were included. CRC-specific and all-cause mortality rate ratios and 95% confidence intervals were calculated by a bivariate random model. (3) Results: 10 RCTs and 47 model studies were retrieved. The pooled CRC-specific mortality rate ratios in RCTs were 0.88 (0.80, 0.96) and 0.76 (0.68, 0.84) for guaiac-based fecal occult blood tests (gFOBT) and single flexible sigmoidoscopy (FS) screening, respectively. For the model studies, the rate ratios were 0.45 (0.39, 0.51) for biennial fecal immunochemical tests (FIT), 0.31 (0.28, 0.34) for biennial gFOBT, 0.61 (0.53, 0.72) for single FS, 0.27 (0.21, 0.35) for 10-yearly colonoscopy, and 0.35 (0.29, 0.42) for 5-yearly FS. The CRC-specific mortality reduction of gFOBT increased with higher adherence in both studies (RCT: 0.78 (0.68, 0.89) vs. 0.92 (0.87, 0.98), model: 0.30 (0.28, 0.33) vs. 0.92 (0.51, 1.63)). Model studies showed a 0.62-1.1% all-cause mortality reduction with single FS screening. (4) Conclusions: Based on RCTs and model studies, biennial FIT/gFOBT, single and 5-yearly FS, and 10-yearly colonoscopy screening significantly reduces CRC-specific mortality. The model estimates are much higher than in RCTs, because the simulated biennial gFOBT assumes higher adherence. The effectiveness of screening increases at younger screening initiation ages and higher adherences.
Keywords: colorectal cancer; meta-analysis; mortality reduction; randomized control trials; screening; simulation models.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- International Agency for Research on Cancer GLOBOCAN 2020. [(accessed on 10 February 2023)]. Available online: https://gco.iarc.fr/today/online-analysis-pie?v=2020&mode=cancer&mode_po....
-
- Allemani C., Matsuda T., Di Carlo V., Harewood R., Matz M., Niksic M., Bonaventure A., Valkov M., Johnson C.J., Esteve J., et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391:1023–1075. doi: 10.1016/S0140-6736(17)33326-3. - DOI - PMC - PubMed
-
- International Agency for Research on Cancer . IARC Handbooks of Cancer Prevention. Volume 17. International Agency for Research on Cancer; Lyon, France: 2019. Colorectal cancer screening; p. 300.
Publication types
LinkOut - more resources
Full Text Sources
