

PSMA-PET Guided Treatment in Prostate Cancer Patients with Oligorecurrent Progression after Previous Salvage Treatment
- PMID: 37046687
- PMCID: PMC10093227
- DOI: 10.3390/cancers15072027
PSMA-PET Guided Treatment in Prostate Cancer Patients with Oligorecurrent Progression after Previous Salvage Treatment
Abstract
Background: Prostate Specific Membrane Antigen-Positron Emission Tomography (PSMA-PET) is used to select recurrent prostate cancer (PCa) patients for metastases-directed therapy (MDT). We aimed to evaluate the oncologic outcomes of second-line PSMA-guided MDT in oligo-recurrent PCa patients.
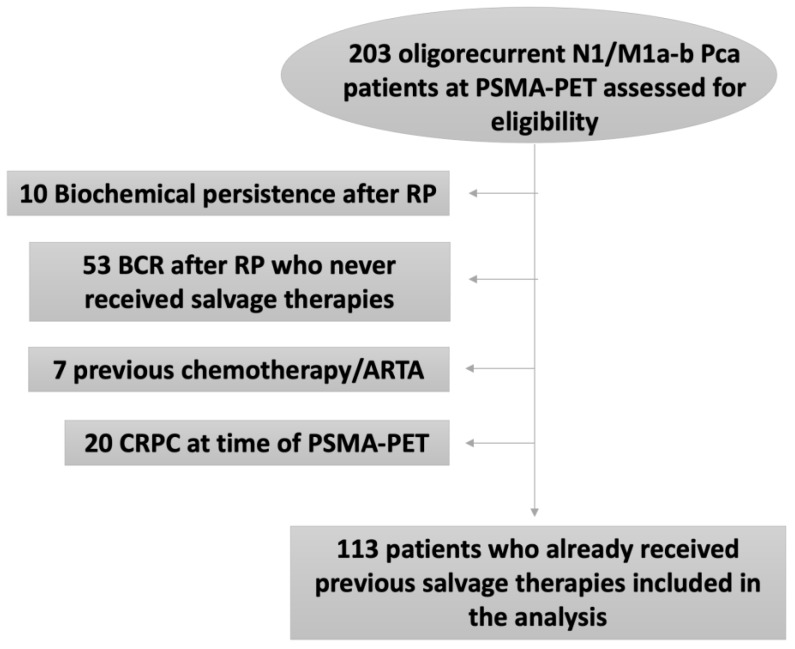
Methods: we performed a retrospective analysis of 113 recurrent PCa after previous radical prostatectomy and salvage therapies with oligorecurrent disease at PSMA-PET (≤3 lesions in N1/M1a-b) in three high-volume European centres. Patients underwent second-line salvage treatments: MDT targeted to PSMA (including surgery and/or radiotherapy), and the conventional approach (observation or Androgen Deprivation Therapy [ADT]). Patients were stratified according to treatments (MDT vs. conventional approach). Patients who underwent MDT were stratified according to stage in PSMA-PET (N1 vs. M1a-b). The primary outcome of the study was Progression-free survival (PFS). Secondary outcomes were Metastases-free survival (MFS) and Castration Resistant PCa free survival (CRPC-FS). Kaplan-Meier analyses assessed PFS, MFS and CRPC-FS. Multivariable Cox regression models identified predictors of progression and metastatic disease.
Results: Overall, 91 (80%) and 22 (20%) patients were treated with MDT and the conventional approach, respectively. The median follow-up after PSMA-PET was 31 months. Patients who underwent MDT had a similar PFS compared to the conventional approach (p = 0.3). Individuals referred to MDT had significantly higher MFS and CRPC-FS compared to those who were treated with the conventional approach (73.5% and 94.7% vs. 30.5% and 79.5%; all p ≤ 0.001). In patients undergoing MDT, no significant differences were found for PFS and MFS according to N1 vs. M1a-b disease, while CRPC-FS estimates were significantly higher in patients with N1 vs. M1a-b (100% vs. 86.1%; p = 0.02). At multivariable analyses, age (HR = 0.96) and ADT during second line salvage treatment (HR = 0.5) were independent predictors of PFS; MDT (HR 0.27) was the only independent predictor of MFS (all p ≤ 0.04) Conclusion: Patients who underwent second-line PSMA-guided MDT experienced higher MFS and CRPC-FS compared to men who received conventional management.
Keywords: PSMA-PET; hormone sensitive prostate cancer; metastasis-directed therapy; oligorecurrent prostate cancer; survival.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures





References
-
- Ost P., Reynders D., Decaestecker K., Fonteyne V., Lumen N., De Bruycker A., Lambert A., Delrue L., Bultijnck R., Claeys T., et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018;36:446–453. doi: 10.1200/JCO.2017.75.4853. - DOI - PubMed
-
- Calais J., Ceci F., Eiber M., AHope T., SHofman M., Rischpler C., Bach-Gansmo T., Nanni C., Savir-Baruch B., Elashoff D., et al. (18)F-fluciclovine PET-CT and (68)Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol. 2019;20:1286–1294. doi: 10.1016/S1470-2045(19)30415-2. - DOI - PMC - PubMed
-
- Perera M., Papa N., Christidis D., Wetherell D., Hofman M.S., Murphy D.G., Bolton D., Lawrentschuk N. Sensitivity, Specificity, and Predictors of Positive 68Ga-Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2016;70:926–937. doi: 10.1016/j.eururo.2016.06.021. - DOI - PubMed
-
- Farolfi A., Ceci F., Castellucci P., Graziani T., Siepe G., Lambertini A., Schiavina R., Lodi F., Morganti A.G., Fanti S., et al. (68)Ga-PSMA-11 PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy and PSA <0.5 ng/ml. Efficacy and impact on treatment strategy. Eur. J. Nucl. Med. Mol. Imaging. 2019;46:11–19. doi: 10.1007/s00259-018-4066-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
