

Comparison of Pathological Outcome and Recurrence Rate between En Bloc Transurethral Resection of Bladder Tumor and Conventional Transurethral Resection: A Meta-Analysis
- PMID: 37046715
- PMCID: PMC10093679
- DOI: 10.3390/cancers15072055
Comparison of Pathological Outcome and Recurrence Rate between En Bloc Transurethral Resection of Bladder Tumor and Conventional Transurethral Resection: A Meta-Analysis
Abstract
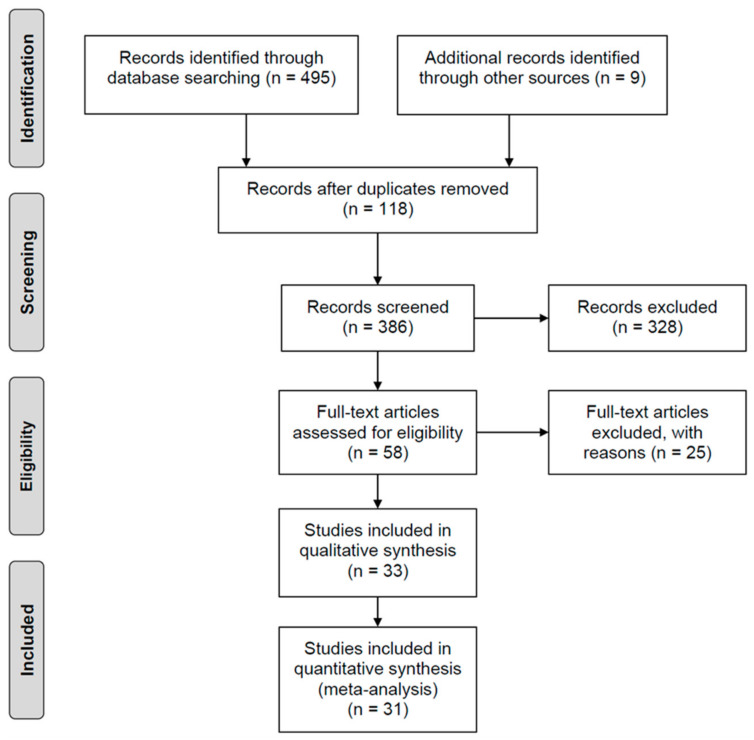
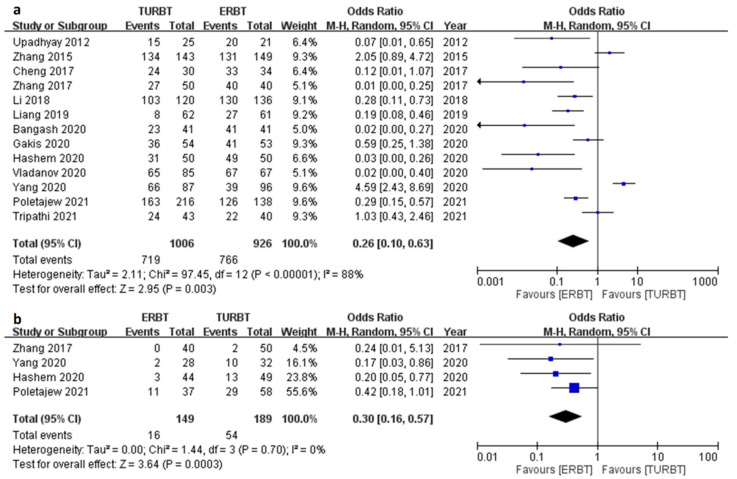
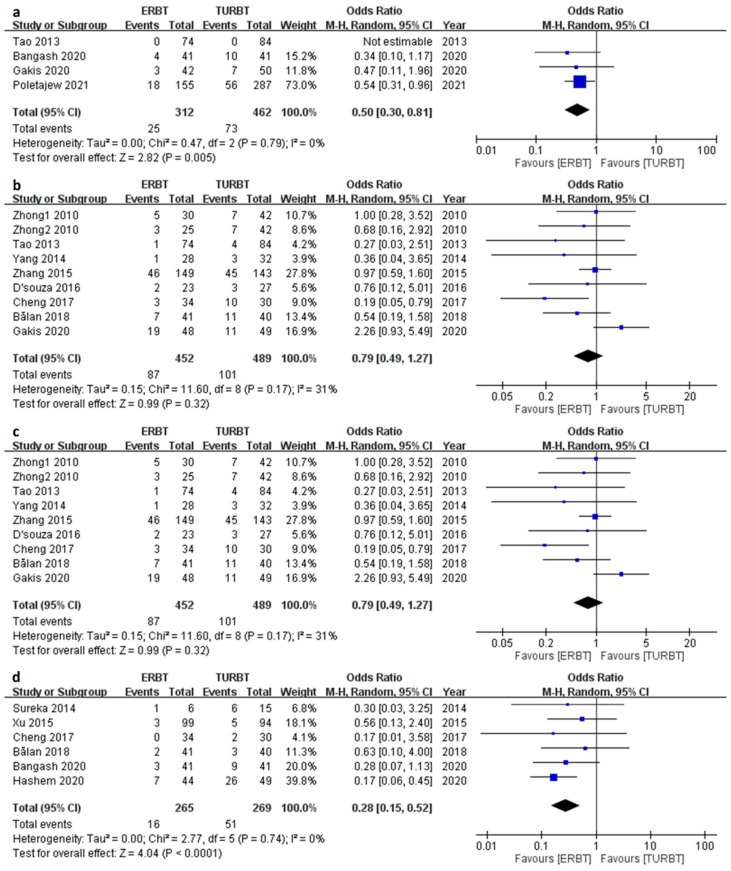
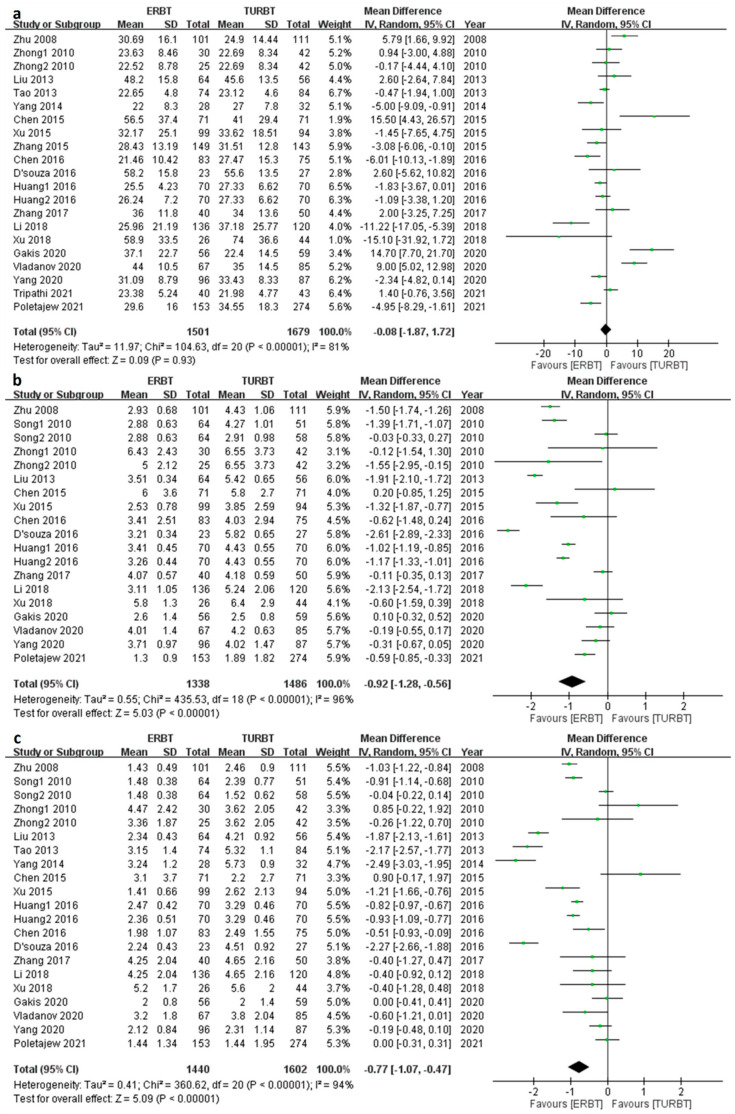
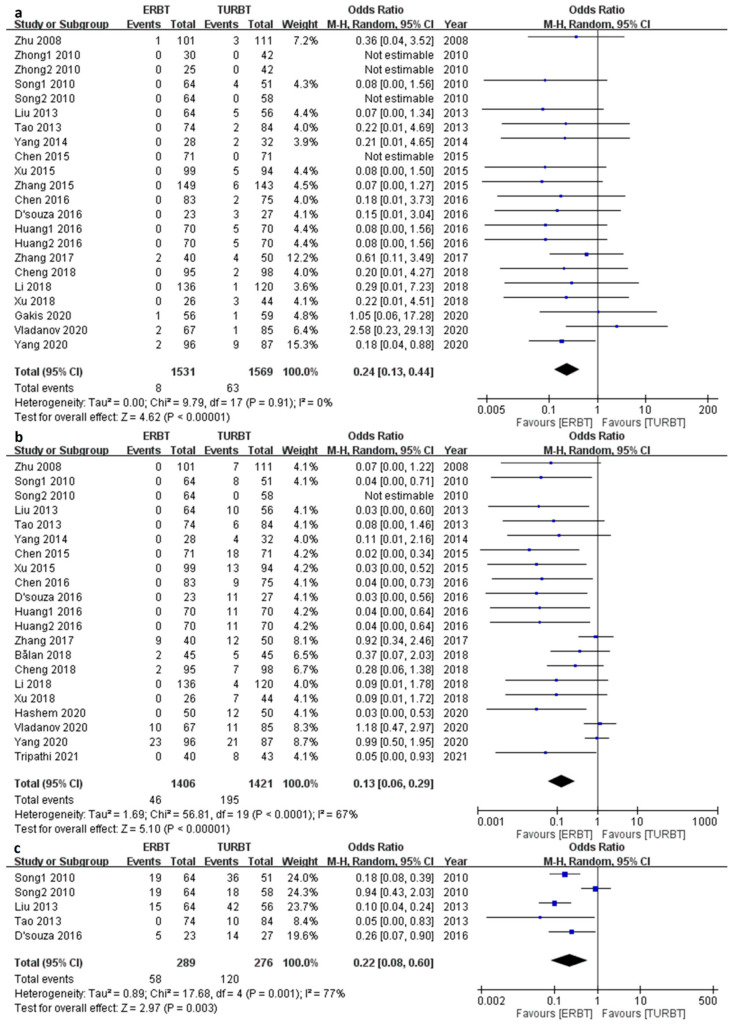
Current treatment for non-muscle invasive bladder cancer (NMIBC) is the conventional transurethral resection of bladder tumor (CTURBT), but the en bloc transurethral resection of bladder tumor (ERBT) has been gaining more attraction in recent years considering better specimen integrity. Thus, we conducted this meta-analysis to compare the safety and efficacy of ERBT versus CTURBT. Trials were collected from an online database. The primary outcomes included identification of detrusor muscle in specimen, residual tumor, 3, 12, and 24-month recurrence rates and same-site recurrence rate. A total of 31 trials were included. The ERBT group had a higher rate of identification of detrusor muscle in specimens (p = 0.003) and lower residual tumor (p < 0.001). Other than that, lower rates of 3-month (p = 0.005) and 24-month recurrence rate (p < 0.001), same-site recurrence rate (p < 0.001) and complications were also observed. For perioperative outcomes, shorter hospitalization time (HT) (p < 0.001), and catheterization time (CT) (p < 0.001) were also revealed in the ERBT group. No significant difference was found in operative time (OT) (p = 0.93). The use of ERBT showed better pathological outcomes and fewer complications, so it could be considered a more effective treatment option for NMIBC.
Keywords: detrusor muscle; en bloc resection of bladder tumor; non-muscle invasive bladder cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Babjuk M., Burger M., Capoun O., Cohen D., Compérat E.M., Escrig J.L.D., Gontero P., Liedberg F., Masson-Lecomte A., Mostafid A.H., et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ) Eur. Urol. 2022;81:75–94. doi: 10.1016/j.eururo.2021.08.010. - DOI - PubMed
-
- Ferro M., Barone B., Crocetto F., Lucarelli G., Busetto G.M., Del Giudice F., Maggi M., Crocerossa F., Cantiello F., Damiano R., et al. Predictive clinico-pathological factors to identify BCG, unresponsive patients, after re-resection for T1 high grade non-muscle invasive bladder cancer. Urol. Oncol. 2022;40:490.e13–490.e20. doi: 10.1016/j.urolonc.2022.05.016. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
