

Selecting the Appropriate Downstaging and Bridging Therapies for Hepatocellular Carcinoma: What Is the Role of Transarterial Radioembolization? A Pooled Analysis
- PMID: 37046783
- PMCID: PMC10093460
- DOI: 10.3390/cancers15072122
Selecting the Appropriate Downstaging and Bridging Therapies for Hepatocellular Carcinoma: What Is the Role of Transarterial Radioembolization? A Pooled Analysis
Abstract
Background: Transarterial radioembolization in HCC for LT as downstaging/bridging has been increasing in recent years but some indication criteria are still unclear.
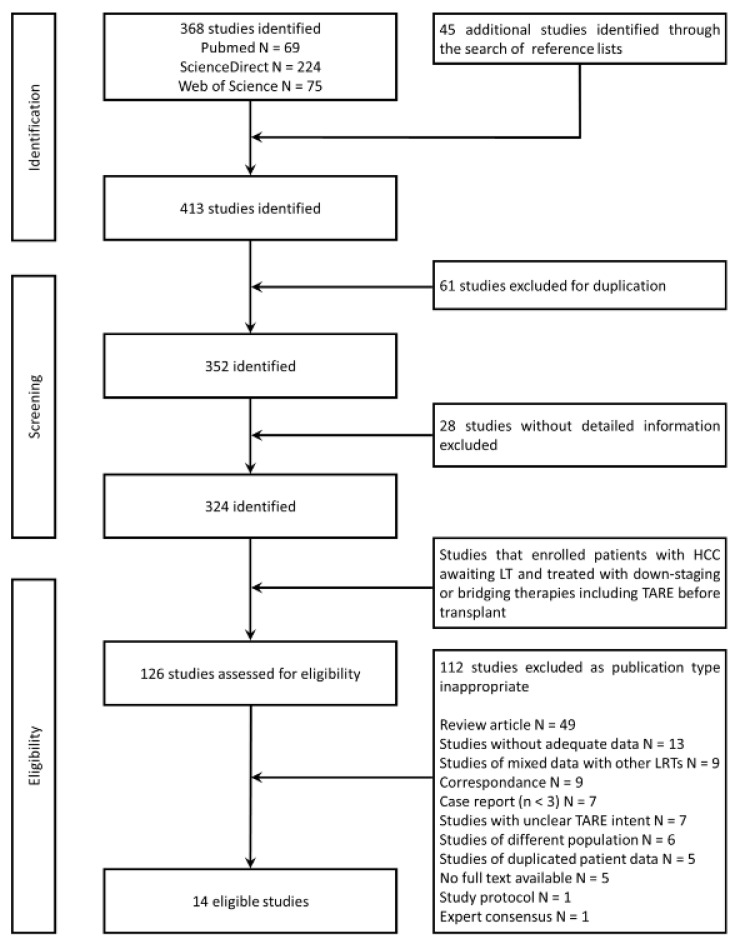
Methods: We conducted a systematic literature search of primary research publications conducted in PubMed, Scopus and ScienceDirect databases until November 2022. Relevant data about patient selection, HCC features and oncological outcomes after TARE for downstaging or bridging in LT were analyzed.
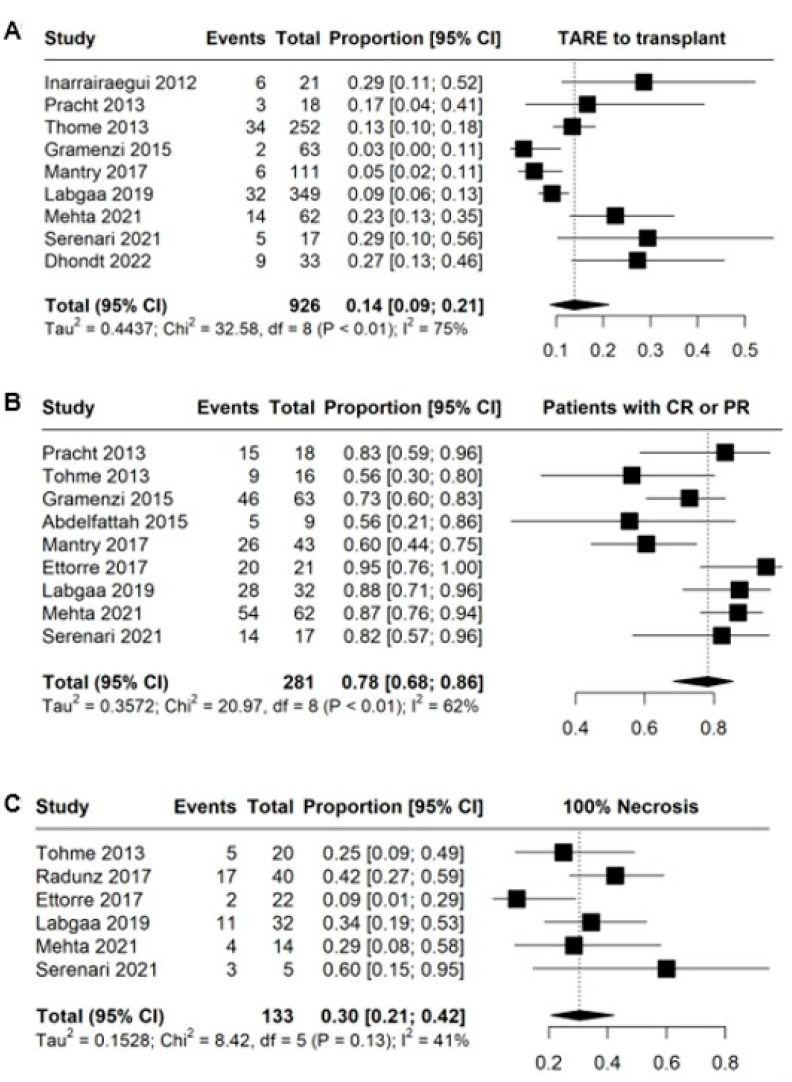
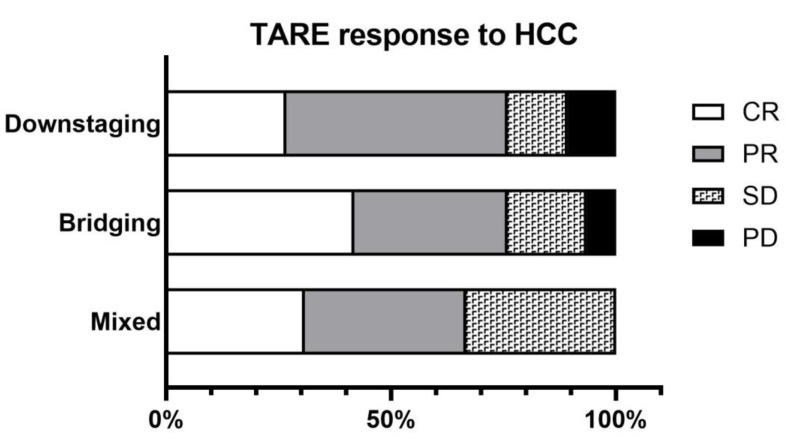
Results: A total of 14 studies were included (7 downstaging, 3 bridging and 4 mixed downstaging and bridging). The proportion of whole liver TARE was between 0 and 1.6%. Multiple TARE interventions were necessary for 16.7% up to 28% of the patients. A total of 55 of 204 patients across all included studies undergoing TARE for downstaging were finally transplanted. The only RCT included presents a higher tumor response with the downstaging rate for LT of TARE than TACE (9/32 vs. 4/34, respectively). Grade 3 or 4 adverse effects rate were detected between 15 and 30% of patients.
Conclusions: TARE is a safe therapeutic option with potential advantages in its capacity to necrotize and reduce the size of the HCC for downstaging or bridging in LT.
Keywords: bridging; downstaging; hepatocellular carcinoma; liver transplant; transarterial radioembolization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Akinyemiju T., Abera S., Ahmed M., Alam N., Alemayohu M.A., Allen C., Al-Raddadi R., Alvis-Guzman N., Amoako Y., Artaman A., et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3:1683–1691. - PMC - PubMed
-
- Kwong A.J., Ghaziani T.T., Yao F., Sze D., Mannalithara A., Mehta N. National Trends and Waitlist Outcomes of Locoregional Therapy Among Liver Transplant Candidates With HCC in the United States. Clin. Gastroenterol. Hepatol. 2022;20:1142–1150.e4. doi: 10.1016/j.cgh.2021.07.048. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
