

Genetics and Epigenetics: Implications for the Life Course of Gestational Diabetes
- PMID: 37047019
- PMCID: PMC10094577
- DOI: 10.3390/ijms24076047
Genetics and Epigenetics: Implications for the Life Course of Gestational Diabetes
Abstract
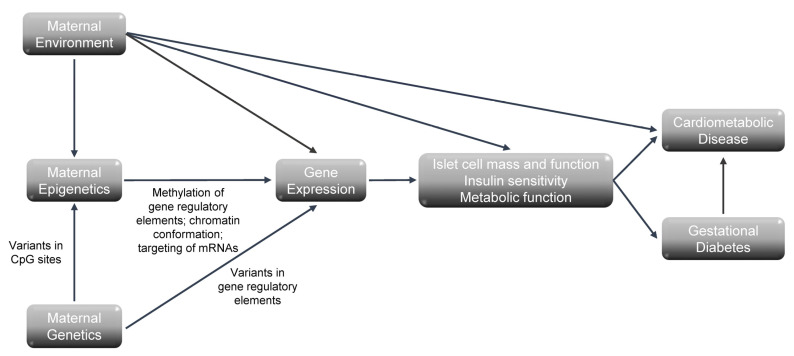
Gestational diabetes (GDM) is one of the most common complications of pregnancy, affecting as many as one in six pregnancies. It is associated with both short- and long-term adverse outcomes for the mother and fetus and has important implications for the life course of affected women. Advances in genetics and epigenetics have not only provided new insight into the pathophysiology of GDM but have also provided new approaches to identify women at high risk for progression to postpartum cardiometabolic disease. GDM and type 2 diabetes share similarities in their pathophysiology, suggesting that they also share similarities in their genetic architecture. Candidate gene and genome-wide association studies have identified susceptibility genes that are shared between GDM and type 2 diabetes. Despite these similarities, a much greater effect size for MTNR1B in GDM compared to type 2 diabetes and association of HKDC1, which encodes a hexokinase, with GDM but not type 2 diabetes suggest some differences in the genetic architecture of GDM. Genetic risk scores have shown some efficacy in identifying women with a history of GDM who will progress to type 2 diabetes. The association of epigenetic changes, including DNA methylation and circulating microRNAs, with GDM has also been examined. Targeted and epigenome-wide approaches have been used to identify DNA methylation in circulating blood cells collected during early, mid-, and late pregnancy that is associated with GDM. DNA methylation in early pregnancy had some ability to identify women who progressed to GDM, while DNA methylation in blood collected at 26-30 weeks gestation improved upon the ability of clinical factors alone to identify women at risk for progression to abnormal glucose tolerance post-partum. Finally, circulating microRNAs and long non-coding RNAs that are present in early or mid-pregnancy and associated with GDM have been identified. MicroRNAs have also proven efficacious in predicting both the development of GDM as well as its long-term cardiometabolic complications. Studies performed to date have demonstrated the potential for genetic and epigenetic technologies to impact clinical care, although much remains to be done.
Keywords: DNA methylation; cardiovascular disease; epigenetics; genetics; gestational diabetes; non-coding RNAs; type 2 diabetes.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
