

Mature Cystic Teratoma: An Integrated Review
- PMID: 37047114
- PMCID: PMC10093990
- DOI: 10.3390/ijms24076141
Mature Cystic Teratoma: An Integrated Review
Abstract
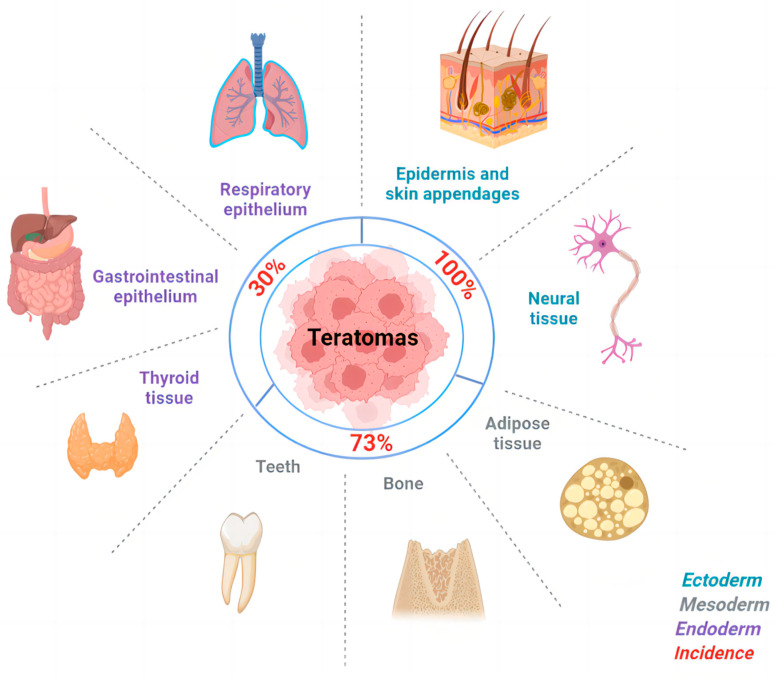
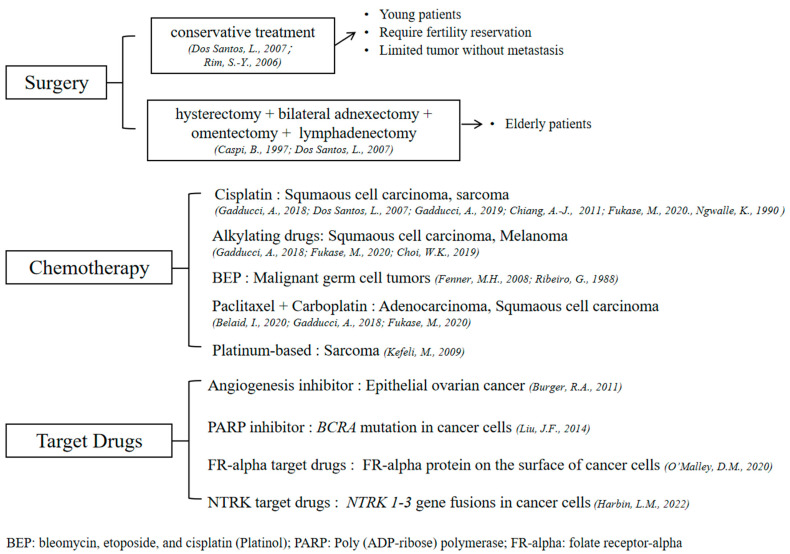
Ovarian dermoid cysts, also called mature cystic teratomas (MCTs), account for 69% of ovarian germ cell tumors in young women. The tumors are formed by tissues derived from three germ layers, and sebaceous materials are most commonly seen. The origin of MCTs is widely considered to be the germ cell origin, which completes meiosis I. The clinical symptoms vary widely, but 20% of tumors could be asymptomatic. The diagnosis of MCTs is usually made without difficulty by ultrasound and confirmed by histopathology post-operatively. The imaging findings have a high diagnostic value. The typical characteristics present in the sonographic images, including a dermoid plug or Rokitansky nodule, are considered strong evidence for a teratoma. Although the malignant transformation of MCTs is rare, it can occur in some cases, especially in women of advanced age. The treatment of MCTs depends on the risk of malignancy, the age of the patient, and the patient's fertility reserve requirement. In this article, we review the epidemiology, clinical symptoms, diagnosis criteria, cellular origin, and treatment of mature cystic teratomas.
Keywords: benign ovarian tumors; germ cell tumors; malignant; mature cystic teratomas; target cancer therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Germ cell tumors of the gonads: a selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues.Mod Pathol. 2005 Feb;18 Suppl 2:S61-79. doi: 10.1038/modpathol.3800310. Mod Pathol. 2005. PMID: 15761467 Review.
-
A curious case of ovarian cysts.JAAPA. 2022 Dec 1;35(12):61-63. doi: 10.1097/01.JAA.0000892764.53306.c4. JAAPA. 2022. PMID: 36412944
-
Mature cystic teratomas arise from meiotic oocytes, but not from pre-meiotic oogonia.Genes Chromosomes Cancer. 2016 Apr;55(4):355-64. doi: 10.1002/gcc.22339. Epub 2016 Jan 21. Genes Chromosomes Cancer. 2016. PMID: 26791142
-
Ovarian Teratoma in Routine Biopsy Material During a Five-Year Period.Acta Clin Croat. 2016 Jun;55(2):265-70. doi: 10.20471/acc.2016.55.02.13. Acta Clin Croat. 2016. PMID: 28394114
-
Follicular variant of papillary thyroid carcinoma arising from a dermoid cyst: a rare malignancy in young women and review of the literature.Taiwan J Obstet Gynecol. 2012 Sep;51(3):421-5. doi: 10.1016/j.tjog.2012.07.019. Taiwan J Obstet Gynecol. 2012. PMID: 23040929 Review.
Cited by
-
An atypical abdominal manifestation of retroperitoneal teratoma: Case report.Int J Surg Case Rep. 2024 Dec;125:110605. doi: 10.1016/j.ijscr.2024.110605. Epub 2024 Nov 15. Int J Surg Case Rep. 2024. PMID: 39580981 Free PMC article.
-
Retroperitoneal cystic mature teratoma in an adult male: A clinical report of one case and review of the literature.Medicine (Baltimore). 2025 Jan 17;104(3):e41284. doi: 10.1097/MD.0000000000041284. Medicine (Baltimore). 2025. PMID: 39833047 Free PMC article. Review.
-
Fetiform teratoma: a systematic review with insights into concepts and controversies in differentiating it from fetus-in-fetu.Pediatr Surg Int. 2025 Jun 14;41(1):170. doi: 10.1007/s00383-025-06087-7. Pediatr Surg Int. 2025. PMID: 40515865 Review.
-
Combined Pharmacological and surgical treatments for recurrent chemical peritonitis due to rupture of a bilateral mature cystic teratoma: a case report.BMC Womens Health. 2025 Apr 11;25(1):172. doi: 10.1186/s12905-025-03719-x. BMC Womens Health. 2025. PMID: 40217218 Free PMC article.
-
Ovarian squamous cell carcinoma: clinicopathological features, prognosis and immunotherapy outcomes.J Gynecol Oncol. 2025 Jul;36(4):e54. doi: 10.3802/jgo.2025.36.e54. Epub 2024 Dec 17. J Gynecol Oncol. 2025. PMID: 39791511 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
