

A PCOS Paradox: Does Inositol Therapy Find a Rationale in All the Different Phenotypes?
- PMID: 37047186
- PMCID: PMC10094056
- DOI: 10.3390/ijms24076213
A PCOS Paradox: Does Inositol Therapy Find a Rationale in All the Different Phenotypes?
Abstract
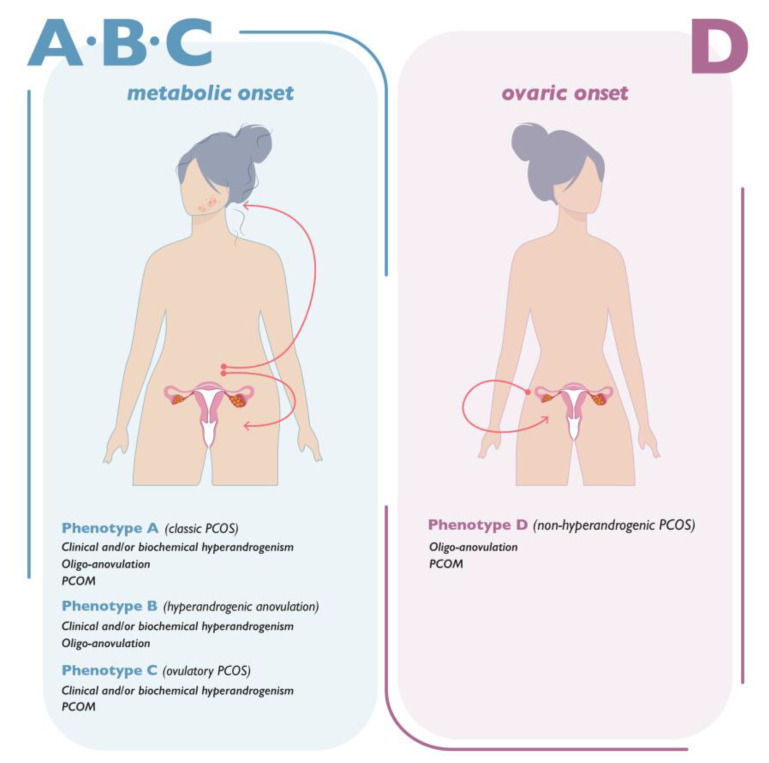
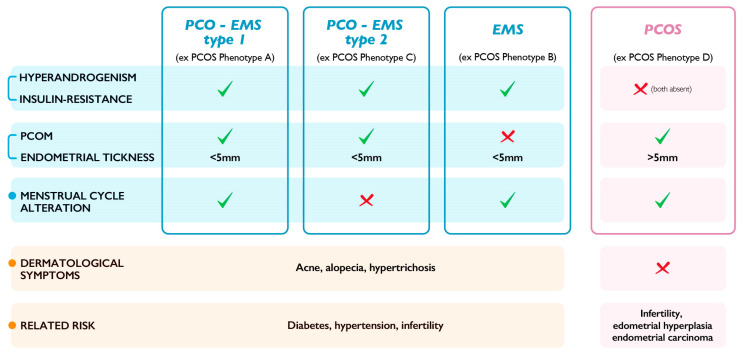
A recent evaluation of the published data regarding the PCOS topic has highlighted a paradox in the definition of this condition. Even though the name of the syndrome refers to ovarian dysfunction, it seems that patients diagnosed with PCOS are more likely affected by an endocrine and metabolic issue. The term PCOS might not be appropriate to indicate the phenotypes described by the Rotterdam criteria, since the only phenotype with a gynecological issue alone is PCOS phenotype D. This novel perspective regarding how PCOS is currently defined leads the way to a reinterpretation of the entire pathological context and the treatment prescribed, such as inositols. A new point of view on the etiopathogenesis of the disease completely changes the current meaning of PCOS and consequently the therapeutic rationale evaluated to date.
Keywords: PCOS; dysmetabolism; endocrine syndrome; myo-inositol; phenotype D.
Conflict of interest statement
V.U., S.D. and M.R. are employed at Lo.Li. Pharma Srl, Rome (Italy).
Figures
References
-
- Stein I.F., Leventhal M.L. Amenorrhea associated with bilateral polycystic ovaries. Am. J. Obstet. Gynecol. 1935;29:181–191. doi: 10.1016/S0002-9378(15)30642-6. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
