

Plasma Proteomics Unveil Novel Immune Signatures and Biomarkers upon SARS-CoV-2 Infection
- PMID: 37047248
- PMCID: PMC10093853
- DOI: 10.3390/ijms24076276
Plasma Proteomics Unveil Novel Immune Signatures and Biomarkers upon SARS-CoV-2 Infection
Abstract
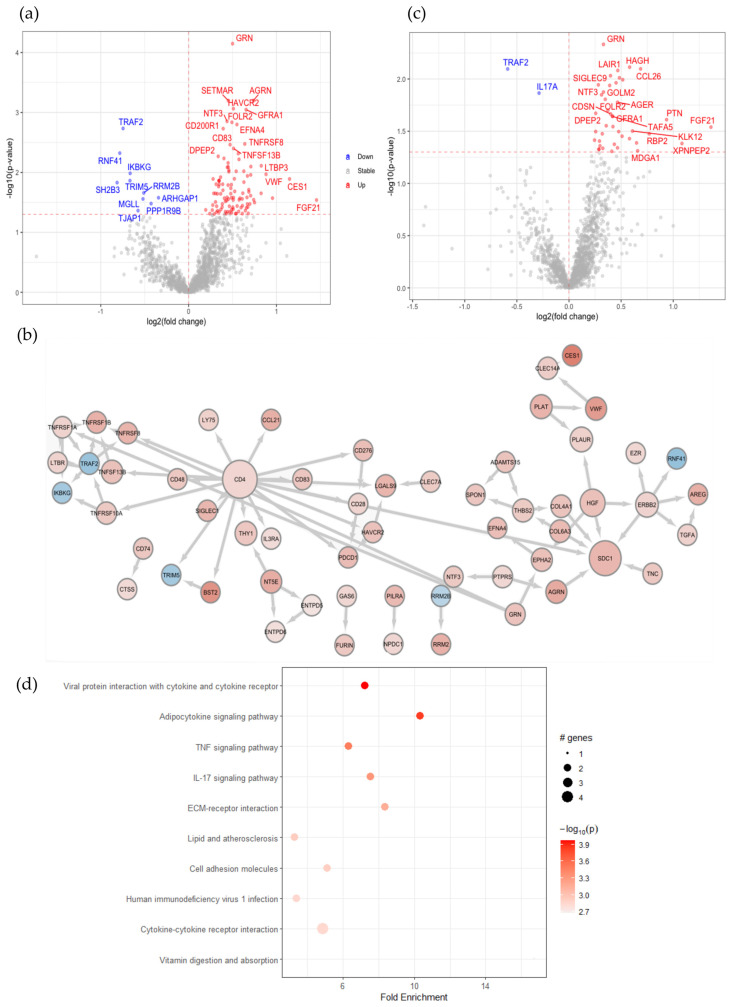
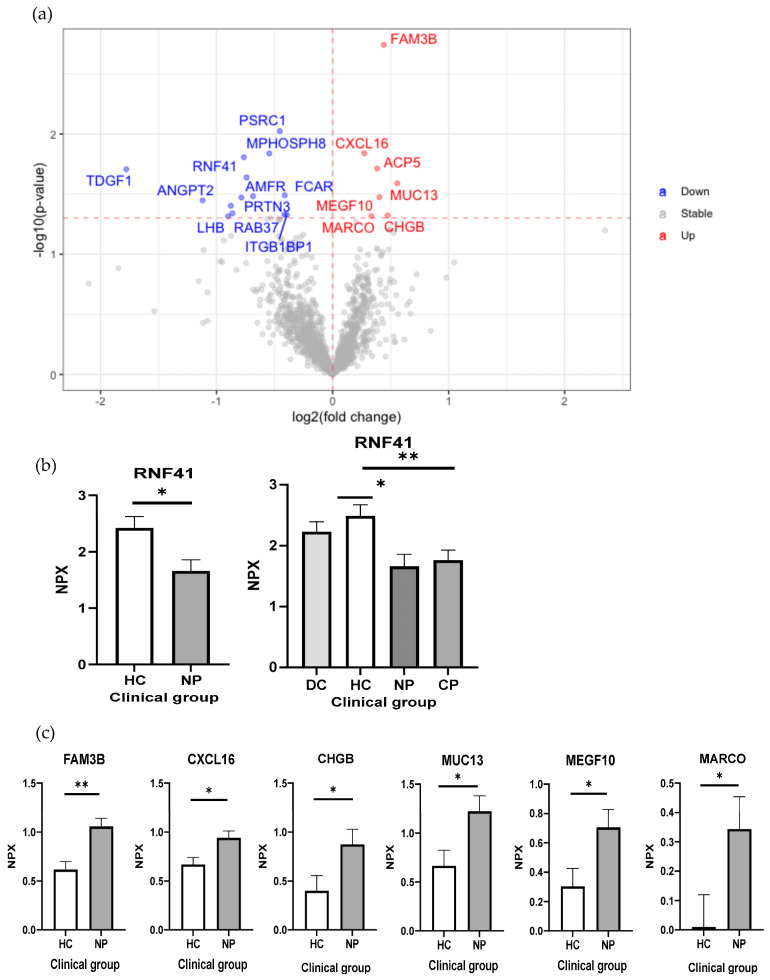
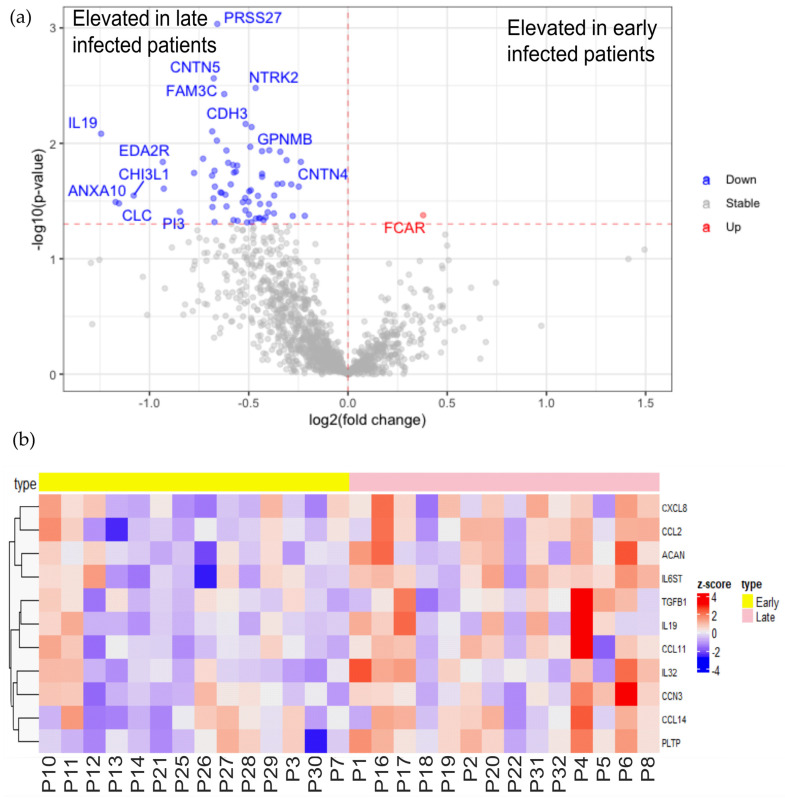
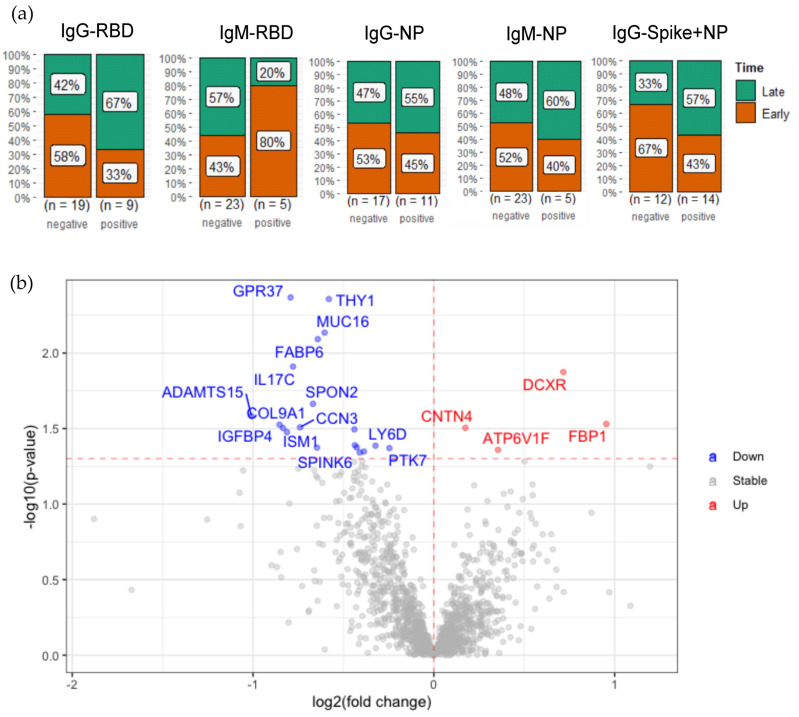
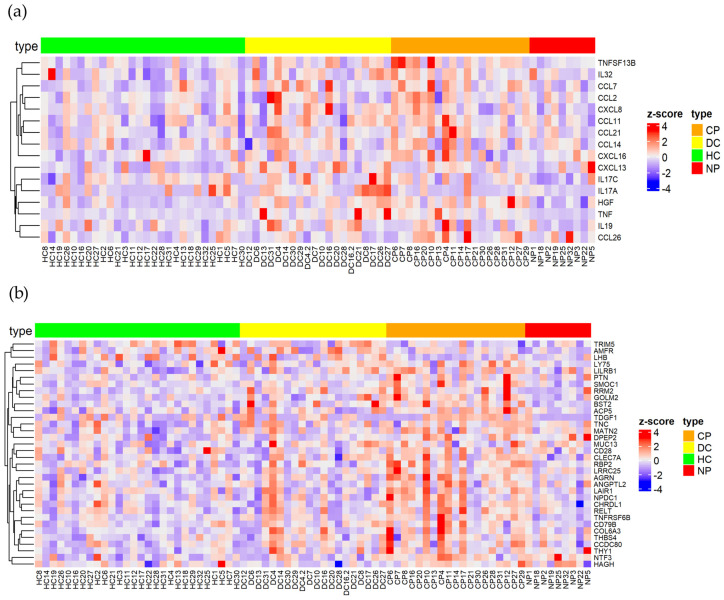
Several elements have an impact on COVID-19, including comorbidities, age and sex. To determine the protein profile changes in peripheral blood caused by a SARS-CoV-2 infection, a proximity extension assay was used to quantify 1387 proteins in plasma samples among 28 Finnish patients with COVID-19 with and without comorbidities and their controls. Key immune signatures, including CD4 and CD28, were changed in patients with comorbidities. Importantly, several unreported elevated proteins in patients with COVID-19, such as RBP2 and BST2, which show anti-microbial activity, along with proteins involved in extracellular matrix remodeling, including MATN2 and COL6A3, were identified. RNF41 was downregulated in patients compared to healthy controls. Our study demonstrates that SARS-CoV-2 infection causes distinct plasma protein changes in the presence of comorbidities despite the interpatient heterogeneity, and several novel potential biomarkers associated with a SARS-CoV-2 infection alone and in the presence of comorbidities were identified. Protein changes linked to the generation of SARS-CoV-2-specific antibodies, long-term effects and potential association with post-COVID-19 condition were revealed. Further study to characterize the identified plasma protein changes from larger cohorts with more diverse ethnicities of patients with COVID-19 combined with functional studies will facilitate the identification of novel diagnostic, prognostic biomarkers and potential therapeutic targets for patients with COVID-19.
Keywords: COVID-19; SARS-CoV-2; biomarker; immune signature; plasma proteomics.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- WHO . COVID-19 Weekly Epidemiological Update. World Health Organization; Geneva, Switzerland: 2022. pp. 1–23.
-
- Bergamaschi L., Mescia F., Turner L., Hanson A.L., Kotagiri P., Dunmore B.J., Ruffieux H., De Sa A., Huhn O., Morgan M.D., et al. Longitudinal analysis reveals that delayed bystander CD8+ T cell activation and early immune pathology distinguish severe COVID-19 from mild disease. Immunity. 2021;54:1257–1275.e8. doi: 10.1016/j.immuni.2021.05.010. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
