

Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack?
- PMID: 37048141
- PMCID: PMC10092948
- DOI: 10.3390/cells12071068
Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack?
Abstract
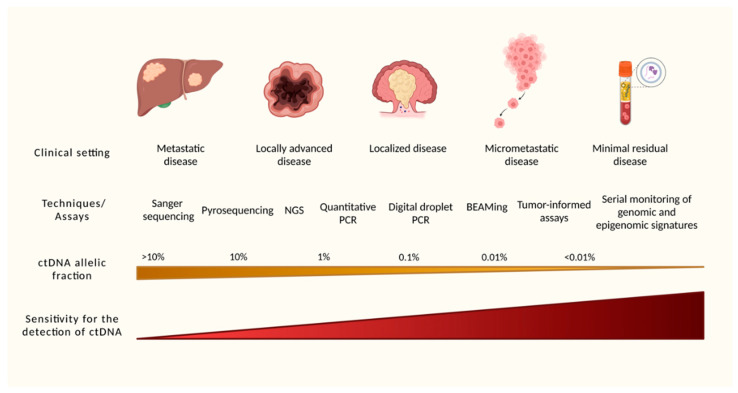
Despite significant advances in the surgical and systemic therapy of colorectal cancer (CRC) in recent decades, recurrence rates remain high. Apart from microsatellite instability status, the decision to offer adjuvant chemotherapy to patients with CRC is solely based on clinicopathologic factors, which offer an inaccurate risk stratification of patients who derive benefit from adjuvant therapy. Owing to the recent improvements of molecular techniques, it has been possible to detect small allelic fractions of circulating tumor DNA (ctDNA), and therefore, to identify patients with minimal residual disease (MRD) after curative-intent therapies. The incorporation of ctDNA identifying MRD in clinical practice may dramatically change the standard of care of CRC, refining the selection of patients who are candidates for escalation and de-escalation of adjuvant chemotherapy, and even for organ-preservation strategies in rectal cancer. In the present review, we describe the current standard of care and the DNA sequencing methodologies and assays, present the data from completed clinical studies and list ongoing potential landmark clinical trials whose results are eagerly awaited, as well as the impact and perspectives for the near future. The discussed data bring optimism for the future of oncologic care through the hope of refined utilization of adjuvant therapies with higher efficacy and safety for patients with both localized and advanced CRC.
Keywords: adjuvant; chemotherapy; circulating tumor DNA; colorectal neoplasms; high-throughput nucleotide sequencing; neoplasm; residual.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
