

Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia
- PMID: 37048577
- PMCID: PMC10095217
- DOI: 10.3390/jcm12072493
Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia
Abstract
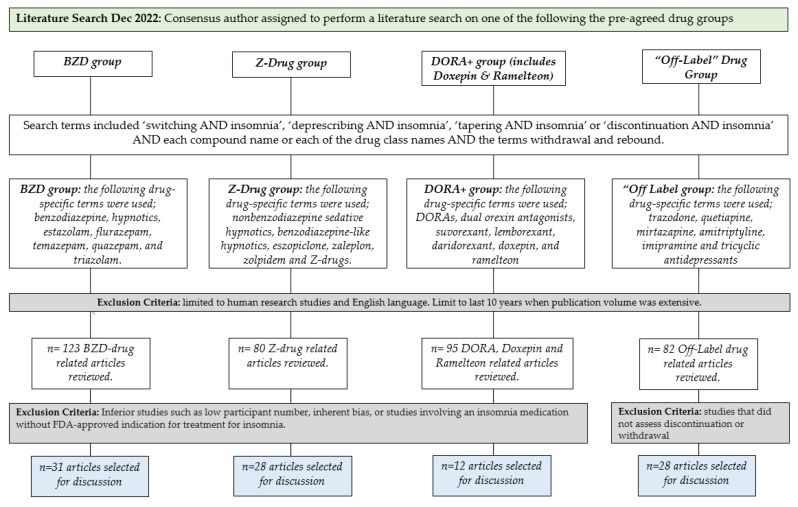
Determining the most effective insomnia medication for patients may require therapeutic trials of different medications. In addition, medication side effects, interactions with co-administered medications, and declining therapeutic efficacy can necessitate switching between different insomnia medications or deprescribing altogether. Currently, little guidance exists regarding the safest and most effective way to transition from one medication to another. Thus, we developed evidence-based guidelines to inform clinicians regarding best practices when deprescribing or transitioning between insomnia medications. Five U.S.-based sleep experts reviewed the literature involving insomnia medication deprescribing, tapering, and switching and rated the quality of evidence. They used this evidence to generate recommendations through discussion and consensus. When switching or discontinuing insomnia medications, we recommend benzodiazepine hypnotic drugs be tapered while additional CBT-I is provided. For Z-drugs zolpidem and eszopiclone (and not zaleplon), especially when prescribed at supratherapeutic doses, tapering is recommended with a 1-2-day delay in administration of the next insomnia therapy when applicable. There is no need to taper DORAs, doxepin, and ramelteon. Lastly, off-label antidepressants and antipsychotics used to treat insomnia should be gradually reduced when discontinuing. In general, offering individuals a rationale for deprescribing or switching and involving them in the decision-making process can facilitate the change and enhance treatment success.
Keywords: deprescribing; hypnotics; insomnia; insomnia medications; switching.
Conflict of interest statement
The authors are solely responsible for the content of this publication and wish to declare the following beyond Idorsia: Watson has served as an advisory consultant for Eisai, Jazz Pharmaceuticals, Harmony Biosciences, Takeda, Johnson and Johnson, Itamar, GlaxoSmithKline, Pfizer and Bayer; Benca has served as a consultant for Eisai, Jazz Pharmaceuticals, Merck, Roche/Genentech, and Sage; Krystal holds the following research grants: Janssen Pharmaceuticals, Axsome Pharmaceutics, Neurocrine Biosciences, Reveal Biosensors, the Ray and Dagmar Dolby Family Fund, and the National Institutes of Health. Krystal has also served as a consultant for the following companies: Adare, Axsome Therapeutics, Big Health, Eisai, Evecxia, Ferring Pharmaceuticals, Galderma, Harmony Biosciences, Janssen Pharmaceuticals, Jazz Pharmaceuticals, Millenium Pharmaceuticals, Merck, Neurocrine Biosciences, Neurawell, Pernix, Otsuka Pharmaceuticals, Sage, Takeda, Angelini; McCall is a clinical advisor for Carelon and receives royalties from Wolters Kluwer; Dr. Neubauer serves as a consultant to Eisai, and he receives royalties from Wolters Kluwer.
Figures
Similar articles
-
Reduction of Sleep Medications via a Combined Digital Insomnia and Pharmacist-Led Deprescribing Intervention: Protocol for a Feasibility Trial.JMIR Res Protoc. 2023 Jul 20;12:e47636. doi: 10.2196/47636. JMIR Res Protoc. 2023. PMID: 37471122 Free PMC article.
-
Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline.Can Fam Physician. 2018 May;64(5):339-351. Can Fam Physician. 2018. PMID: 29760253 Free PMC article.
-
Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline.J Clin Sleep Med. 2017 Feb 15;13(2):307-349. doi: 10.5664/jcsm.6470. J Clin Sleep Med. 2017. PMID: 27998379 Free PMC article.
-
Insomnia in Elderly Patients: Recommendations for Pharmacological Management.Drugs Aging. 2018 Sep;35(9):791-817. doi: 10.1007/s40266-018-0569-8. Drugs Aging. 2018. PMID: 30058034 Review.
-
Deprescribing antipsychotics for behavioural and psychological symptoms of dementia and insomnia: Evidence-based clinical practice guideline.Can Fam Physician. 2018 Jan;64(1):17-27. Can Fam Physician. 2018. PMID: 29358245 Free PMC article. Review.
Cited by
-
Comment on Watson et al. Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia. J. Clin. Med. 2023, 12, 2493.J Clin Med. 2025 Feb 28;14(5):1634. doi: 10.3390/jcm14051634. J Clin Med. 2025. PMID: 40095607 Free PMC article.
-
A retrospective clinical practice study comparing the usefulness of dual-orexin receptor antagonists and a melatonin receptor agonist in patients switching from long-term benzodiazepine receptor agonists.J Clin Sleep Med. 2024 Apr 1;20(4):603-613. doi: 10.5664/jcsm.10946. J Clin Sleep Med. 2024. PMID: 38063235 Free PMC article.
-
Efficacy and Safety of Transitioning to Lemborexant from Z-drug, Suvorexant, and Ramelteon in Japanese Insomnia Patients: An Open-label, Multicenter Study.Adv Ther. 2024 Apr;41(4):1728-1745. doi: 10.1007/s12325-024-02811-2. Epub 2024 Mar 9. Adv Ther. 2024. PMID: 38460107 Free PMC article. Clinical Trial.
-
Addressing Sleep Disorders in Psychiatry: Comparing the Use of Melatonin, Trazodone, and Doxepin.Cureus. 2024 Dec 28;16(12):e76507. doi: 10.7759/cureus.76507. eCollection 2024 Dec. Cureus. 2024. PMID: 39872559 Free PMC article.
-
Orexinergic Receptor Antagonists as a New Therapeutic Target to Overcome Limitations of Current Pharmacological Treatment of Insomnia Disorder.Actas Esp Psiquiatr. 2024 Apr;52(2):172-182. doi: 10.62641/aep.v52i2.1659. Actas Esp Psiquiatr. 2024. PMID: 38622003 Free PMC article.
References
-
- Sateia M.J., Buysse D.J., Krystal A.D., Neubauer D.N., Heald J.L. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: An american academy of sleep medicine clinical practice guideline. J. Clin. Sleep Med. 2017;13:307–349. doi: 10.5664/jcsm.6470. - DOI - PMC - PubMed
-
- Espie C.A., Pawlecki B., Waterfield D., Fitton K., Radocchia M., Luik A.I. Insomnia symptoms and their association with workplace productivity: Cross-sectional and pre-post intervention analyses from a large multinational manufacturing company. Sleep Health. 2018;4:307–312. doi: 10.1016/j.sleh.2018.03.003. - DOI - PubMed
