

Diagnostic Accuracy of Endoscopic Ultrasonography in Selecting Patients for Endoscopic Submucosal Dissection for Early Gastrointestinal Neoplasms
- PMID: 37048589
- PMCID: PMC10094822
- DOI: 10.3390/jcm12072505
Diagnostic Accuracy of Endoscopic Ultrasonography in Selecting Patients for Endoscopic Submucosal Dissection for Early Gastrointestinal Neoplasms
Abstract
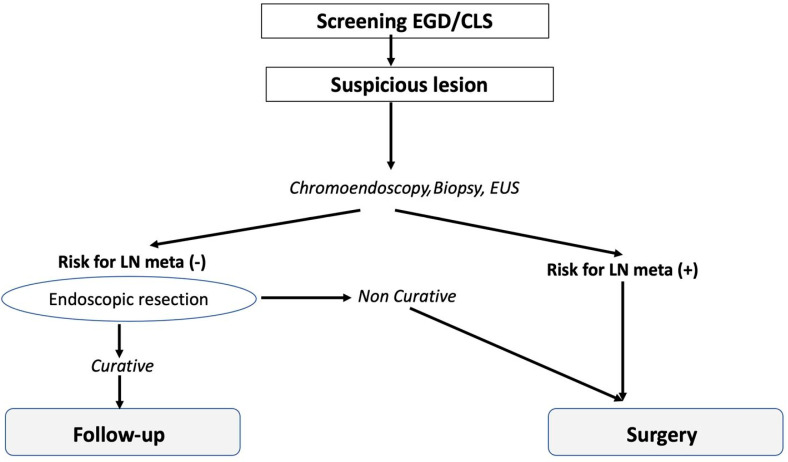
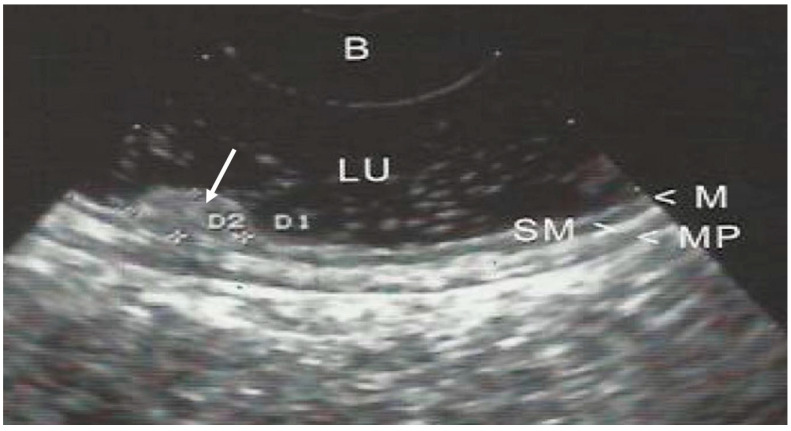
Tumor invasion depth and lymph node metastasis determine the prognosis of gastrointestinal (GI) neoplasms. GI neoplasms limited to mucosa (m1 or m2) and superficial submucosa (sm1) can be treated effectively with minimally invasive endoscopic therapy, while the deep invasion of the submucosa (sm2 or sm3) is associated with lymph node metastasis, and surgical resection is required. Correct staging is therefore crucial for preoperative evaluation and planning. Endoscopic ultrasonography (EUS) can be used to detect the depth of invasion due to its close proximity to the lesion. The diagnostic accuracy of EUS, when compared to conventional endoscopic staging, is debated as it can under- or overstage the lesion. We aim in this study to determine if EUS can accurately differentiate mucosal from submucosal GI neoplasms to select patients with early GI lesions for endoscopic submucosal dissection (ESD) or surgery. From March 2014 to February 2022, 293 patients with early superficial GI neoplasms were admitted to our endoscopic unit for EUS staging. To evaluate the accuracy of EUS, we compared the preoperative EUS findings with the definitive histopathologic findings on the resected specimen. Overall, 242 of 293 lesions were correctly staged by EUS (82.59%). In the evaluation of submucosal invasion or deeper, EUS understaged 38 of 293 (12.96%) and overstaged 13 of 293 (4.43%) lesions. EUS has excellent accuracy in staging superficial GI neoplasms; its use is highly recommended before ESD since it can also detect lymph node metastases around the lesions, thus changing the indication from ESD to surgery.
Keywords: ESD; endoscopic ultrasonography; gastrointestinal neoplasms; prognosis; staging; subepithelial lesion.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Liu L., Hofstetter W., Rashid A., Swisher S.G., Correa A.M., Ajani J.A., Hamilton S.R., Wu T.T. Significance of the depth of tumor invasion and lymph node metastasis in superficially invasive (T1) esophageal adenocarcinoma. Am. J. Surg. Pathol. 2005;29:1079–1085. doi: 10.1097/01.pas.0000168175.63782.9e. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
