

Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery
- PMID: 37048600
- PMCID: PMC10094905
- DOI: 10.3390/jcm12072516
Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery
Abstract
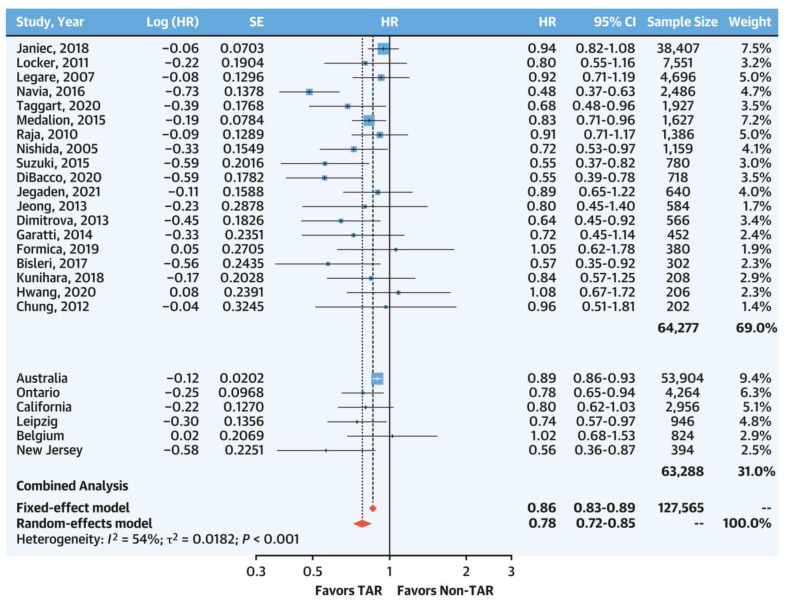
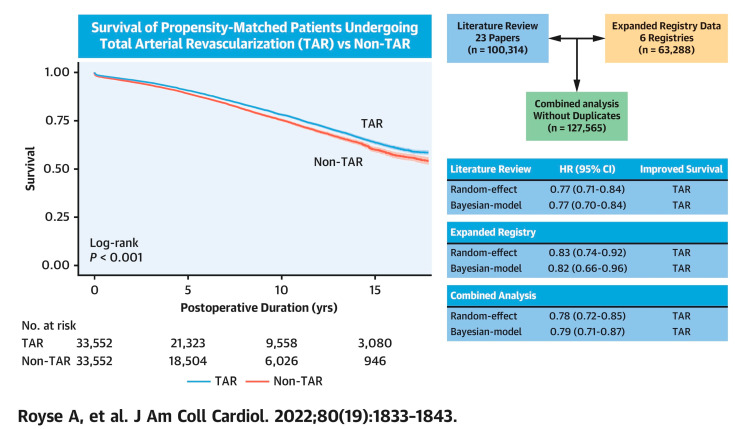
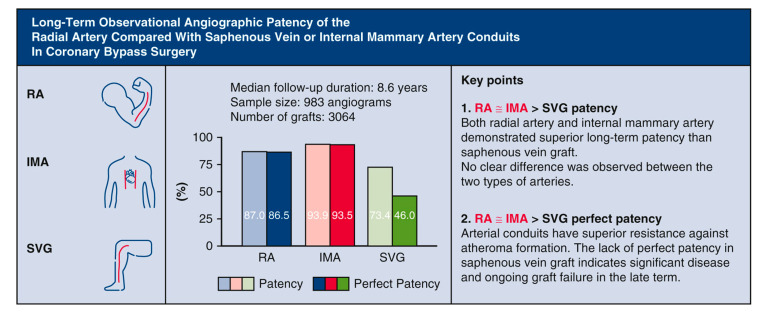
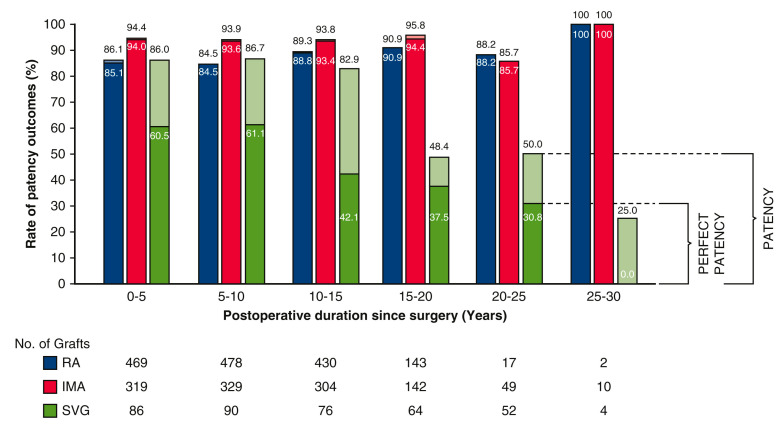
Coronary surgery provides better long-term outcomes than percutaneous coronary intervention. Conventional practice is to use a single arterial conduit supplemented by saphenous vein grafts. The use of multiple arterial revascularization (MAG), or exclusive arterial revascularization (TAR), however, is reported as having improved late survival. Survival is a surrogate for graft failure that may lead to premature death, and improved survival reflects fewer graft failures in the non-conventional strategy groups. The reasons for not using MAG or TAR may be due to perceived technical difficulties, a lack of definitive large-scale randomized evidence, a lack of confidence in arterial conduits, or resources or time constraints. Most people consider radial artery (RA) grafting to be new, with use representing approximately 2-5% worldwide, despite select centers reporting routine use in most patients for decades with improved results. In conclusion, the current body of evidence supports more extensive use of total and multiple arterial revascularization procedures in the absence of contraindications.
Keywords: coronary artery bypass grafting; internal mammary artery; multiple arterial grafting; radial artery; total arterial revascularization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Thygesen K., Alpert J.S., Jaffe A.S., Simoons M.L., Chaitman B.R., White H.D., the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Thygesen K., Alpert J.S. Third universal definition of myocardial infarction. Eur. Heart J. 2012;33:2551–2567. doi: 10.1093/eurheartj/ehs184. - DOI - PubMed
-
- Serruys P.W., Morice M.C., Kappetein A.P., Colombo A., Holmes D.R., Mack M.J., Ståhle E., Feldman T.E., van den Brand M., Bass E.J., et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009;360:961–972. doi: 10.1056/NEJMoa0804626. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
