

It Is Always the Same-A Complication Classification following Angular Stable Plating of Proximal Humeral Fractures
- PMID: 37048639
- PMCID: PMC10095119
- DOI: 10.3390/jcm12072556
It Is Always the Same-A Complication Classification following Angular Stable Plating of Proximal Humeral Fractures
Abstract
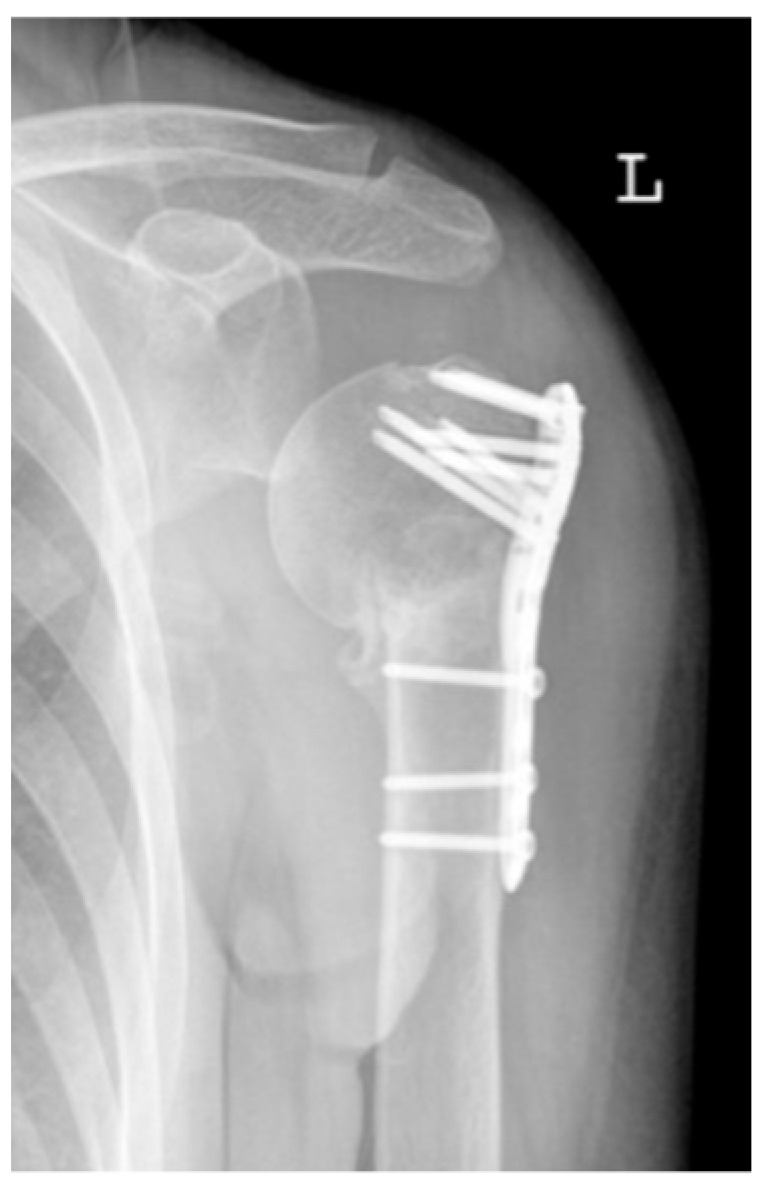
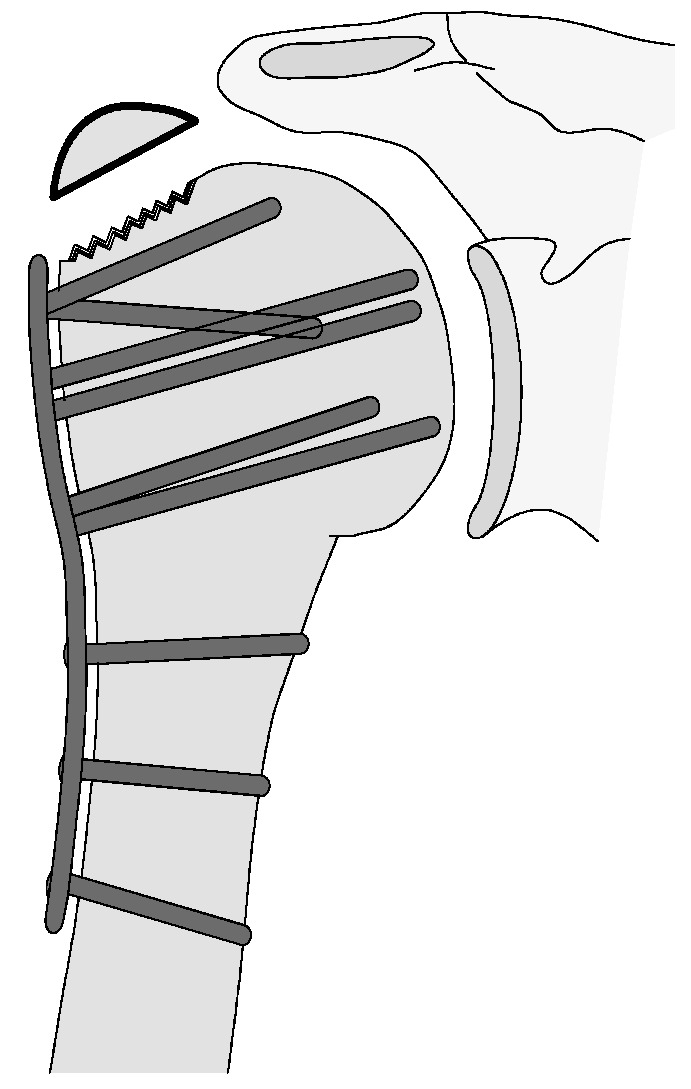
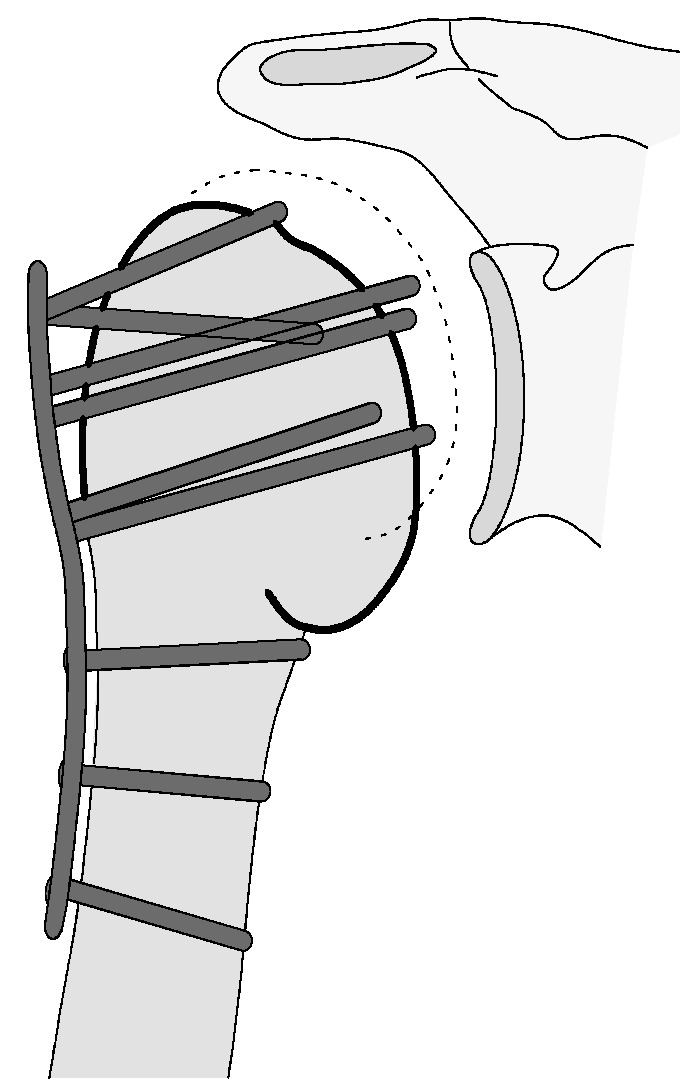
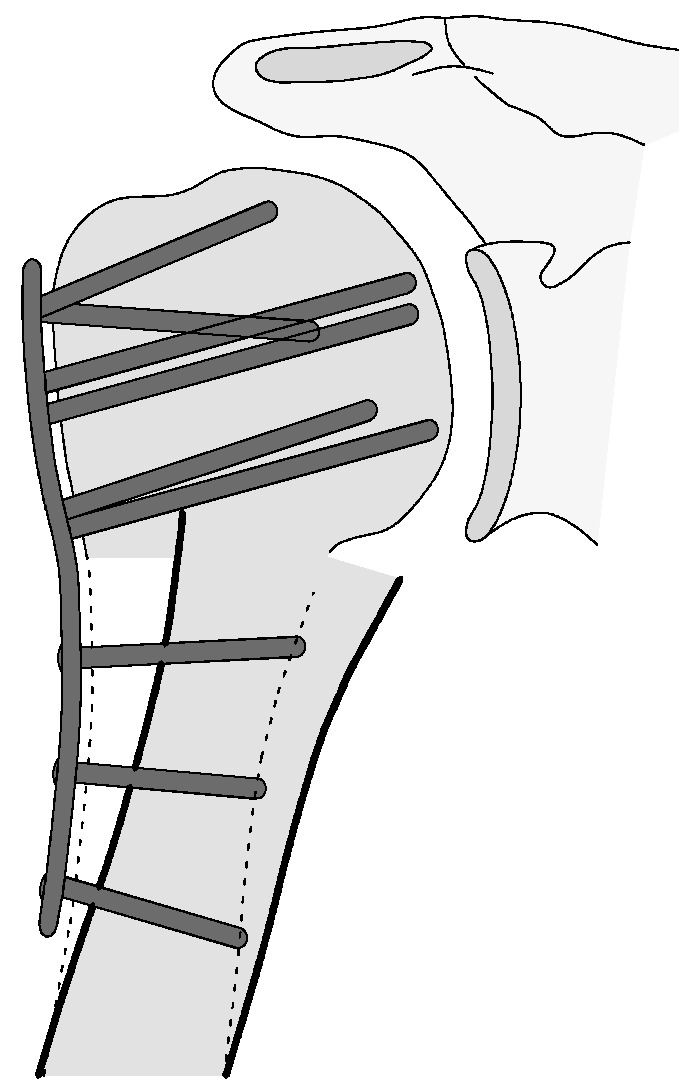
The aim of this study was to create a novel complication classification for osteosynthesis-related complications following angular stable plating of the proximal humerus subsuming the influence of these complications on clinical outcome in relation to fracture morphology and consequent revision strategies. A total of 1047 proximal humerus fractures with overall 193 osteosynthesis-associated complications (24.5%) were included. The following complication types could be clarified: complication Type 1 is defined by mild varus (<20°) or valgus displacement of the humeral head without resulting in a screw cutout through the humeral head cortex. Type 2a is defined by varus displacement (<20°) of the humeral head associated with screw cutout through the humeral head cortex. Type 2b complication is limited to displacement of the greater tuberosity, lesser tuberosity, or both tuberosities. Complication Type 2c is defined by severe varus dislocation (>20°) of the humeral head with screw cutout at the humeral head cortex. Complication Type 3 describes a displacement of the angular stable plate in the humeral shaft region with associated shaft-sided screw cutout, while the position of the humeral head remains static. Complication Type 4 is characterized by the occurrence of AVN with or without glenoidal affection (4a/b). Clinical outcome according to the constant score was mainly affected by type 2-4, leading to a deteriorated result. Depending on the type of complication, specific revision strategies can be considered. Additionally, more complex fracture patterns fostered the incidence of complications.
Keywords: angular stable plating locking plate osteosynthesis; complication classification; complications; constant score; functional outcome; mid-term; proximal humeral fracture.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






















References
LinkOut - more resources
Full Text Sources
