

Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage
- PMID: 37048667
- PMCID: PMC10095006
- DOI: 10.3390/jcm12072585
Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage
Abstract
Objective: Acute hydrocephalus is a common complication in patients with aneurysmal subarachnoid hemorrhage (SAH). Several ventricular indices have been introduced to enable measurements of ventricular morphology. Previously, researchers have showed their diagnostic value for various neurological disorders. In this study, we evaluated the association between ventricular indices and the clinical course, occurrence of complications and outcome of SAH.
Methods: A total of 745 SAH patients with available early admission computed tomography scans were included in the analyses. Six ventricular indices (bifrontal, bicaudate, ventricular and third ventricle ratios and Evans' and Huckman's indices) were measured. Primary endpoints included the occurrence of cerebral infarctions, in-hospital mortality and a poor outcome at 6 months. Secondary endpoints included different adverse events in the course of SAH. Clinically relevant cut-offs for the indices were determined using receiver operating curves. Univariate analyses were performed. Multivariate analyses were conducted on significant findings in a stepwise backward regression model.
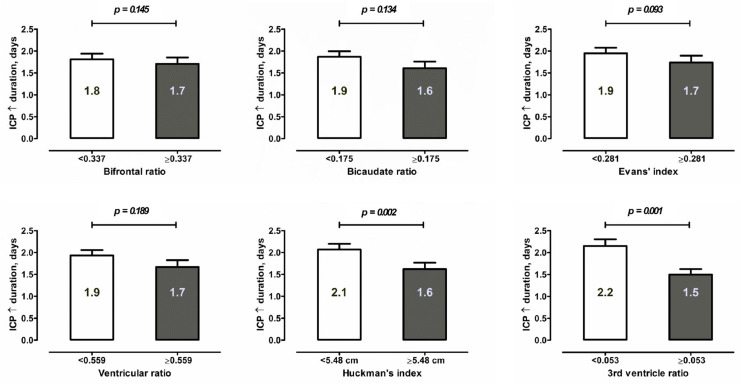
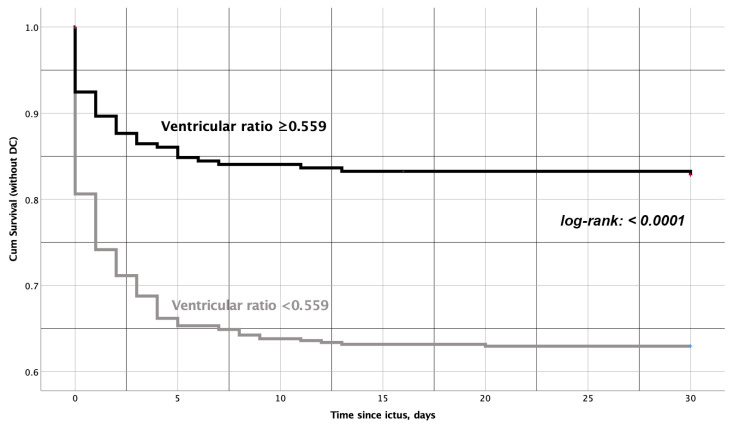
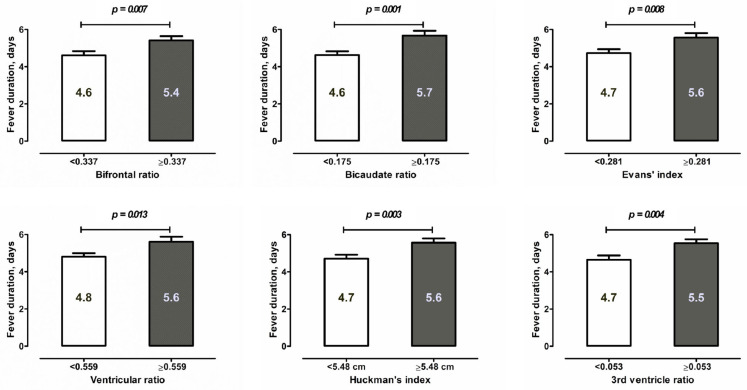
Results: The higher the values of the ventricular indices were and the older the patient was, the higher the WFNS and Fisher's scores were, and the lower the SEBES score was at admission. Patients with larger ventricles showed a shorter duration of intracranial pressure increase > 20 mmHg and required decompressive craniectomy less frequently. Ventricular indices were independently associated with the parameters of inflammatory response after SAH (C-reactive protein in serum and interleukin-6 in cerebrospinal fluid and fever). Finally, there were independent correlations between larger ventricles and all the primary endpoints.
Conclusions: The lower risk of intracranial pressure increase and absence of an association with vasospasm or systemic infections during SAH, and the poorer outcome in individuals with larger ventricles might be related to a more pronounced neuroinflammatory response after aneurysmal bleeding. These observations might be helpful in the development of specific medical and surgical treatment strategies for SAH patients depending on the initial ventricle measurements.
Keywords: decompressive craniectomy; inflammation; marker; subarachnoid hemorrhage; ventricular measurements.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The value of ventricular measurements in the prediction of shunt dependency after aneurysmal subarachnoid hemorrhage.Acta Neurochir (Wien). 2023 Jun;165(6):1545-1555. doi: 10.1007/s00701-023-05595-6. Epub 2023 May 2. Acta Neurochir (Wien). 2023. PMID: 37127799 Free PMC article.
-
Subarachnoid Hemorrhage Early Brain Edema Score (SEBES) as a radiographic marker of clinically relevant intracranial hypertension and unfavorable outcome after subarachnoid hemorrhage.Eur J Neurol. 2021 Dec;28(12):4051-4059. doi: 10.1111/ene.15033. Epub 2021 Aug 4. Eur J Neurol. 2021. PMID: 34293828
-
Comparing radiographic scores for prediction of complications and outcome of aneurysmal subarachnoid hemorrhage: Which performs best?Eur J Neurol. 2023 Mar;30(3):659-670. doi: 10.1111/ene.15634. Epub 2022 Nov 29. Eur J Neurol. 2023. PMID: 36371646
-
Effect of statin treatment on vasospasm-related morbidity and functional outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2017 Aug;127(2):291-301. doi: 10.3171/2016.5.JNS152900. Epub 2016 Oct 7. J Neurosurg. 2017. PMID: 27715439
-
Risk Factors for Cerebral Vasospasm Following Aneurysmal Subarachnoid Hemorrhage: A Review of the Literature.World Neurosurg. 2016 Jan;85:56-76. doi: 10.1016/j.wneu.2015.08.052. Epub 2015 Sep 3. World Neurosurg. 2016. PMID: 26342775 Review.
References
-
- Evans W.J. An encephalographic ratio for estimating ventricular enlargement and cerebral atrophy. Arch. Neurol. Psychiatry. 1942;47:931–937. doi: 10.1001/archneurpsyc.1942.02290060069004. - DOI
-
- Nakajima M., Yamada S., Miyajima M., Ishii K., Kuriyama N., Kazui H., Kanemoto H., Suehiro T., Yoshiyama K., Kameda M., et al. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurol. Med. Chir. 2021;61:63–97. doi: 10.2176/nmc.st.2020-0292. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
