

Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation
- PMID: 37048813
- PMCID: PMC10095385
- DOI: 10.3390/jcm12072730
Electrical Storm Has Worse Prognosis Compared to Sustained Ventricular Tachycardia after VT Ablation
Abstract
Background: Electrical storm (ES) represents a serious heart rhythm disorder. This study investigates the impact of ES on acute ablation success and long-term outcomes after VT ablation compared to non-ES patients.
Methods: In this large single-centre study, patients presenting with ES and undergoing VT ablation from June 2018 to April 2021 were compared to patients undergoing VT ablation due to ventricular tachyarrhythmias but without ES. The primary prognostic outcome was VT recurrence, and secondary endpoints were rehospitalization rates and cardiovascular mortality, all after a median follow-up of 22 months.
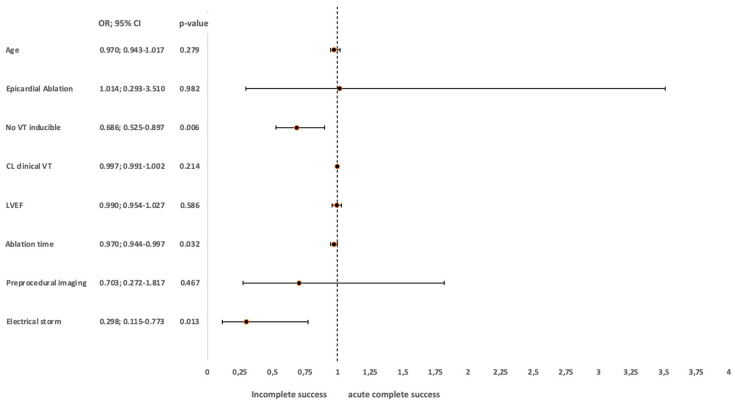
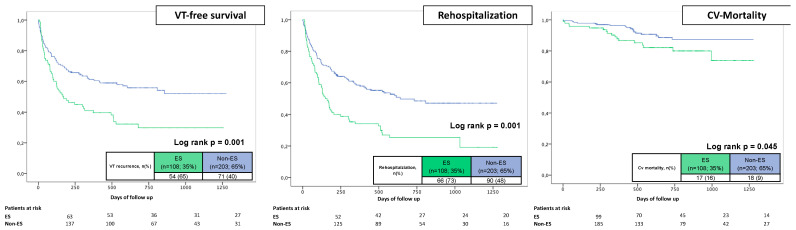
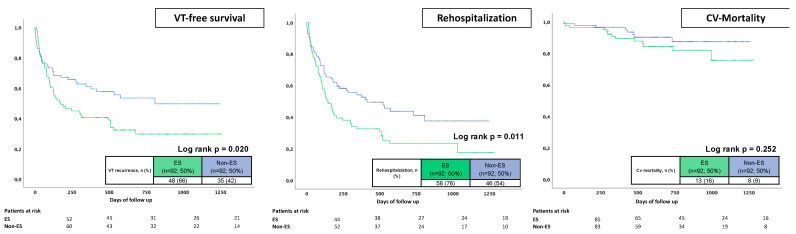
Results: A total of 311 patients underwent a first VT ablation due to ventricular tachyarrhythmias and were included (63 ± 14 years; 86% male). Of these, 108 presented with ES. In the ES cohort, dilated cardiomyopathy as underlying heart disease was significantly higher (p = 0.008). Major complications were equal across both groups (all p > 0.05). Ablation of the clinical VT was achieved in 94% of all patients (p > 0.05). Noninducibility of any VT was achieved in 91% without ES and in 76% with ES (p = 0.001). Patients with ES revealed increased VT recurrence rates during follow-up (65% vs. 40%; log rank p = 0.001; HR 1.841, 95% CI 1.289-2.628; p = 0.001). Furthermore, ES patients suffered from increased rehospitalization rates (73% vs. 48%; log rank p = 0.001; HR 1.948, 95% CI 1.415-2.682; p = 0.001) and cardiovascular mortality (18% vs. 9%; log rank p = 0.045; HR 1.948, 95% CI 1.004-3.780; p = 0.049). After multivariable adjustment, ES was a strong independent predictor of VT recurrence and rehospitalization rates, but not for mortality. In a propensity score-matched cohort, patients with ES still had a higher risk of VT recurrences and rehospitalizations compared to non-ES patients.
Conclusions: VT ablation in patients with ES is challenging and these patients reveal the highest risk for recurrent VTs, rehospitalization and cardiovascular mortality. These patients need close follow-ups and optimal guideline-directed therapy.
Keywords: MACE; acute heart failure; coronary artery disease; electrical storm; hospitalization; mortality; sudden cardiac death.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Villacastin J., Almendral J., Arenal A., Albertos J., Ormaetxe J., Peinado R., Bueno H., Merino J.L., Pastor A., Medina O., et al. Incidence and clinical significance of multiple consecutive, appropriate, high-energy discharges in patients with implanted cardioverter-defibrillators. Circulation. 1996;93:753–762. doi: 10.1161/01.CIR.93.4.753. - DOI - PubMed
-
- Credner S.C., Klingenheben T., Mauss O., Sticherling C., Hohnloser S.H. Electrical storm in patients with transvenous implantable cardioverter-defibrillators: Incidence, management and prognostic implications. J. Am. Coll. Cardiol. 1998;32:1909–1915. doi: 10.1016/S0735-1097(98)00495-1. - DOI - PubMed
-
- Verma A., Kilicaslan F., Marrouche N.F., Minor S., Khan M., Wazni O., Burkhardt J.D., Belden W.A., Cummings J.E., Abdul-Karim A., et al. Prevalence, predictors, and mortality significance of the causative arrhythmia in patients with electrical storm. J. Cardiovasc. Electrophysiol. 2004;15:1265–1270. doi: 10.1046/j.1540-8167.2004.04352.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
