

Vitamin D and Calcium Supplementation and Urolithiasis: A Controversial and Multifaceted Relationship
- PMID: 37049567
- PMCID: PMC10096570
- DOI: 10.3390/nu15071724
Vitamin D and Calcium Supplementation and Urolithiasis: A Controversial and Multifaceted Relationship
Abstract
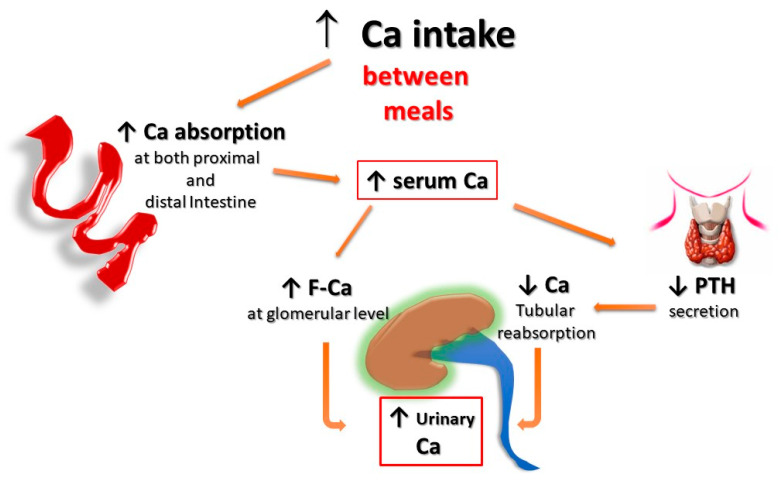
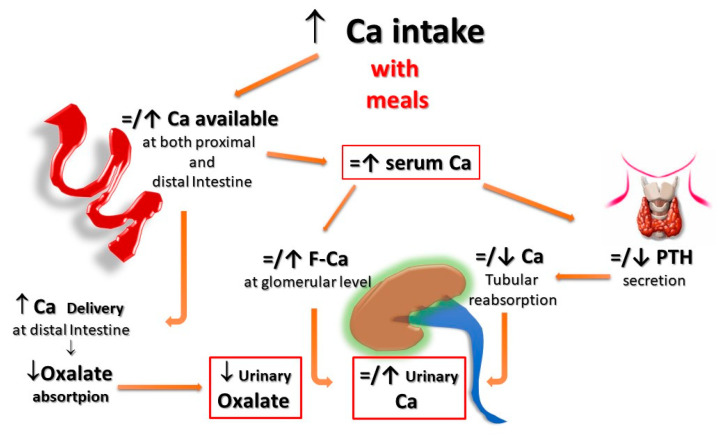
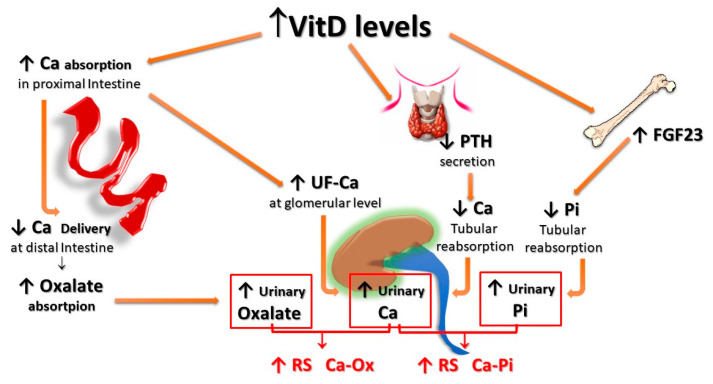
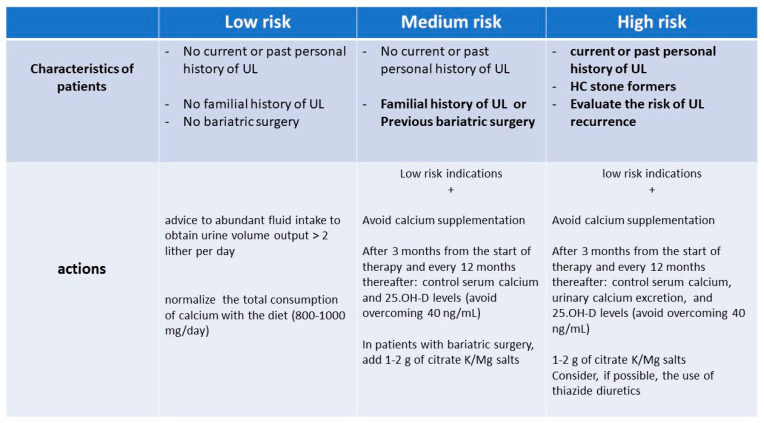
Patients with urolithiasis, and particularly those with hypercalciuria, frequently have a marked reduction of bone mineral content up to the levels of osteoporosis, with a significant increase in bone fracture risk. For these reasons, the indication to prescribe vitamin D and/or calcium supplementations is very frequent in such patients. On the other hand, both calcium supplementation, and even more vitamin D therapy, can worsen the risk of developing urolithiasis by increasing calcium, phosphate, and oxalate urinary excretion. Despite the clinical and practical relevance of this issue, the evidence on this topic is scarce and contradictory. Therefore, some concerns exist about how and whether to prescribe such supplements to a patient with a history of kidney stones. In this narrative review, we resume some pivotal pathophysiological concepts strictly related to the dealt topic, and we draw some considerations and personal opinions on the pros and cons of such prescriptions. Finally, we share with the reader our pragmatic algorithm for handling the urolithiasis risk in patients who have strong indications to be prescribed vitamin D and calcium supplementations.
Keywords: calcium; chronic kidney disease; dietary supplementation; urolithiasis; vitamin D.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
