

Is Autologous Fecal Microbiota Transfer after Exclusive Enteral Nutrition in Pediatric Crohn's Disease Patients Rational and Feasible? Data from a Feasibility Test
- PMID: 37049583
- PMCID: PMC10096730
- DOI: 10.3390/nu15071742
Is Autologous Fecal Microbiota Transfer after Exclusive Enteral Nutrition in Pediatric Crohn's Disease Patients Rational and Feasible? Data from a Feasibility Test
Abstract
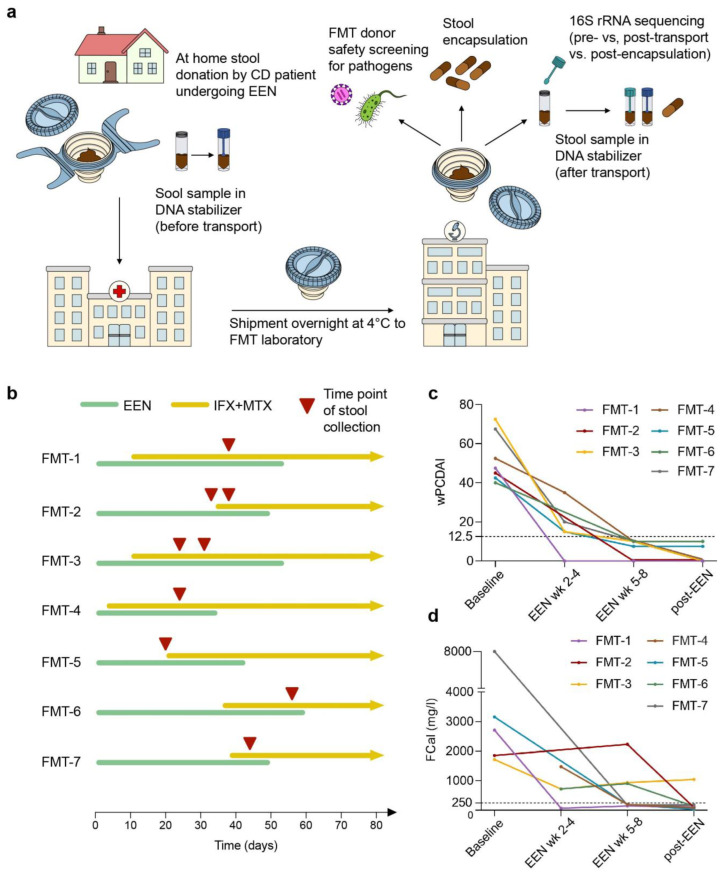
Background: Exclusive enteral nutrition (EEN) is a highly effective therapy for remission induction in pediatric Crohn's disease (CD), but relapse rates after return to a regular diet are high. Autologous fecal microbiota transfer (FMT) using stool collected during EEN-induced clinical remission might represent a novel approach to maintaining the benefits of EEN.
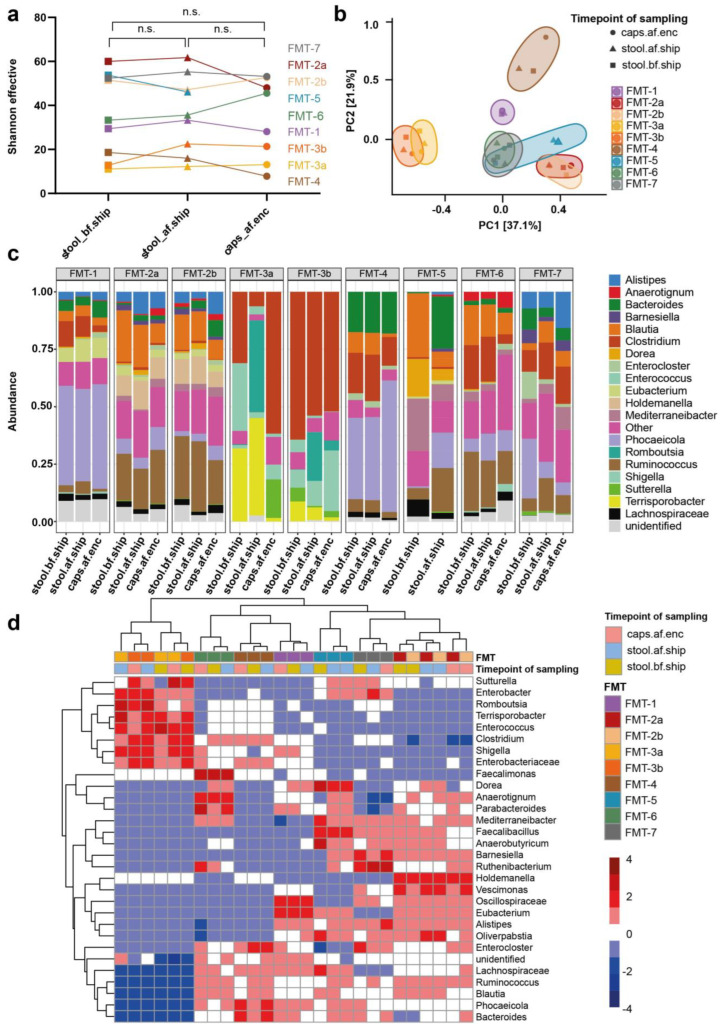
Methods: Pediatric CD patients provided fecal material at home, which was shipped at 4 °C to an FMT laboratory for FMT capsule generation and extensive pathogen safety screening. The microbial community composition of samples taken before and after shipment and after encapsulation was characterized using 16S rRNA amplicon sequencing.
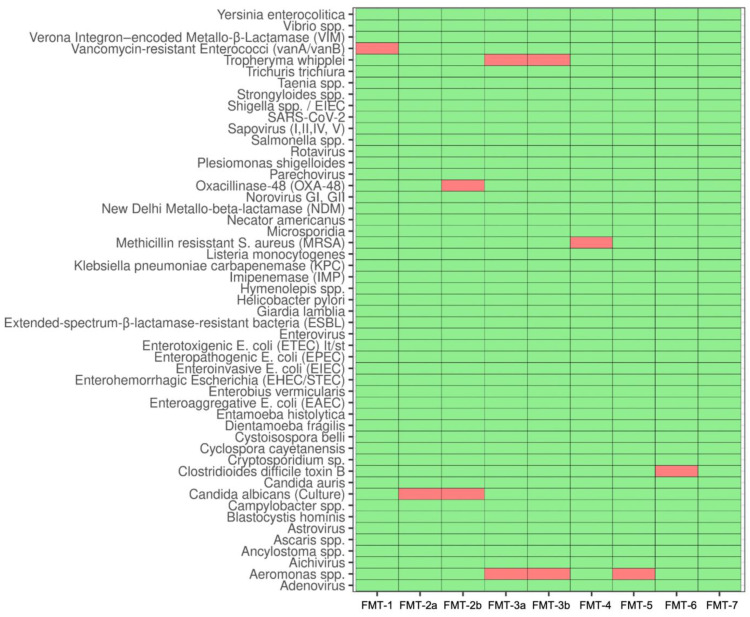
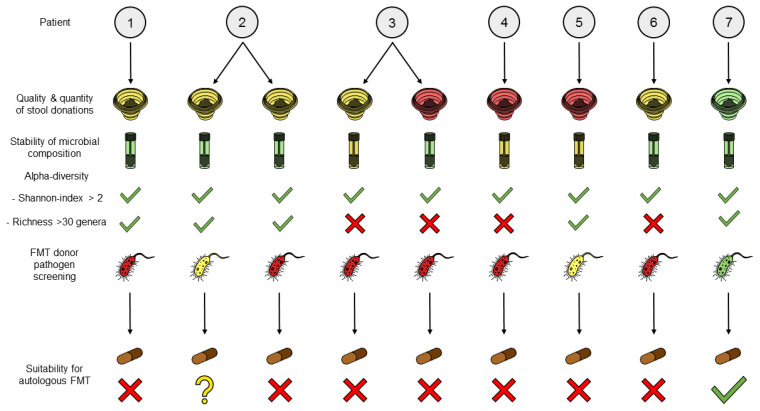
Results: Seven pediatric patients provided fecal material for nine test runs after at least three weeks of nutritional therapy. FMT capsules were successfully generated in 6/8 deliveries, but stool weight and consistency varied widely. Transport and processing of fecal material into FMT capsules did not fundamentally change microbial composition, but microbial richness was <30 genera in 3/9 samples. Stool safety screening was positive for potential pathogens or drug resistance genes in 8/9 test runs.
Conclusions: A high pathogen burden, low-diversity microbiota, and practical deficiencies of EEN-conditioned fecal material might render autologous capsule-FMT an unsuitable approach as maintenance therapy for pediatric CD patients.
Keywords: Crohn’s disease; autologous FMT; exclusive enteral nutrition; fecal microbiota transfer; pediatric IBD.
Conflict of interest statement
T.S. received speaker fees from MSD and Nutricia (Danone). K.N. collaborates with Hipp (Pfaffenhofen, Germany) about novel probiotic strains. The rest of the authors declare that they have no potential conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Repeated and multiple fecal microbiota transplantations plus partial enteral nutrition as the first-line treatment in active pediatric Crohn's disease.Front Cell Infect Microbiol. 2023 Feb 23;13:1083236. doi: 10.3389/fcimb.2023.1083236. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 36909725 Free PMC article.
-
Bacterial Taxa and Functions Are Predictive of Sustained Remission Following Exclusive Enteral Nutrition in Pediatric Crohn's Disease.Inflamm Bowel Dis. 2020 Jun 18;26(7):1026-1037. doi: 10.1093/ibd/izaa001. Inflamm Bowel Dis. 2020. PMID: 31961432 Free PMC article.
-
Treatment of Active Crohn's Disease With Exclusive Enteral Nutrition Diminishes the Immunostimulatory Potential of Fecal Microbial Products.Inflamm Bowel Dis. 2024 Dec 5;30(12):2457-2466. doi: 10.1093/ibd/izae124. Inflamm Bowel Dis. 2024. PMID: 38982655 Free PMC article.
-
Exclusive enteral nutrition versus corticosteroids for treatment of pediatric Crohn's disease: a meta-analysis.World J Pediatr. 2019 Feb;15(1):26-36. doi: 10.1007/s12519-018-0204-0. Epub 2019 Jan 21. World J Pediatr. 2019. PMID: 30666565 Free PMC article. Review.
-
Exclusive Enteral Nutrition Induces Remission in Pediatric Crohn's Disease via Modulation of the Gut Microbiota.Biomed Res Int. 2017;2017:8102589. doi: 10.1155/2017/8102589. Epub 2017 Oct 16. Biomed Res Int. 2017. PMID: 29124070 Free PMC article. Review.
Cited by
-
Validation methods for encapsulated faecal microbiota transplantation: a scoping review.Therap Adv Gastroenterol. 2025 Feb 8;18:17562848251314820. doi: 10.1177/17562848251314820. eCollection 2025. Therap Adv Gastroenterol. 2025. PMID: 39926318 Free PMC article. Review.
-
The current landscape of fecal microbiota transplantation in treating inflammatory bowel disease.Transl Gastroenterol Hepatol. 2025 Jun 11;10:55. doi: 10.21037/tgh-24-138. eCollection 2025. Transl Gastroenterol Hepatol. 2025. PMID: 40755720 Free PMC article. Review.
-
The practice of fecal microbiota transplantation in inflammatory bowel disease.Intest Res. 2024 Jan;22(1):44-64. doi: 10.5217/ir.2023.00085. Epub 2023 Nov 21. Intest Res. 2024. PMID: 37981746 Free PMC article. Review.
References
-
- Kelly C.R., Yen E.F., Grinspan A.M., Kahn S.A., Atreja A., Lewis J.D., Moore T.A., Rubin D.T., Kim A.M., Serra S., et al. Fecal Microbiota Transplantation Is Highly Effective in Real-World Practice: Initial Results From the FMT National Registry. Gastroenterology. 2021;160:183–192.e3. doi: 10.1053/j.gastro.2020.09.038. - DOI - PMC - PubMed
-
- Aggarwala V., Mogno I., Li Z., Yang C., Britton G.J., Chen-Liaw A., Mitcham J., Bongers G., Gevers D., Clemente J.C., et al. Precise Quantification of Bacterial Strains after Fecal Microbiota Transplantation Delineates Long-Term Engraftment and Explains Outcomes. Nat. Microbiol. 2021;6:1309–1318. doi: 10.1038/s41564-021-00966-0. - DOI - PMC - PubMed
-
- Staley C., Kaiser T., Vaughn B.P., Graiziger C., Hamilton M.J., Kabage A.J., Khoruts A., Sadowsky M.J. Durable Long-Term Bacterial Engraftment Following Encapsulated Fecal Microbiota Transplantation To Treat Clostridium Difficile Infection. mBio. 2019;10:e01586-19. doi: 10.1128/mBio.01586-19. - DOI - PMC - PubMed
-
- Moayyedi P., Surette M.G., Kim P.T., Libertucci J., Wolfe M., Onischi C., Armstrong D., Marshall J.K., Kassam Z., Reinisch W., et al. Fecal Microbiota Transplantation Induces Remission in Patients With Active Ulcerative Colitis in a Randomized Controlled Trial. Gastroenterology. 2015;149:102–109.e6. doi: 10.1053/j.gastro.2015.04.001. - DOI - PubMed
-
- Paramsothy S., Kamm M.A., Kaakoush N.O., Walsh A.J., van den Bogaerde J., Samuel D., Leong R.W.L., Connor S., Ng W., Paramsothy R., et al. Multidonor Intensive Faecal Microbiota Transplantation for Active Ulcerative Colitis: A Randomised Placebo-Controlled Trial. Lancet. 2017;389:1218–1228. doi: 10.1016/S0140-6736(17)30182-4. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
