

Factors Associated with the Non-Exacerbator Phenotype of Chronic Obstructive Pulmonary Disease
- PMID: 37051115
- PMCID: PMC10084935
- DOI: 10.2147/COPD.S392070
Factors Associated with the Non-Exacerbator Phenotype of Chronic Obstructive Pulmonary Disease
Abstract
Background: Patients with chronic obstructive pulmonary disease (COPD) and no exacerbations may need less maintenance treatment and follow-up. The aim was to identify factors associated with a non-exacerbator COPD phenotype.
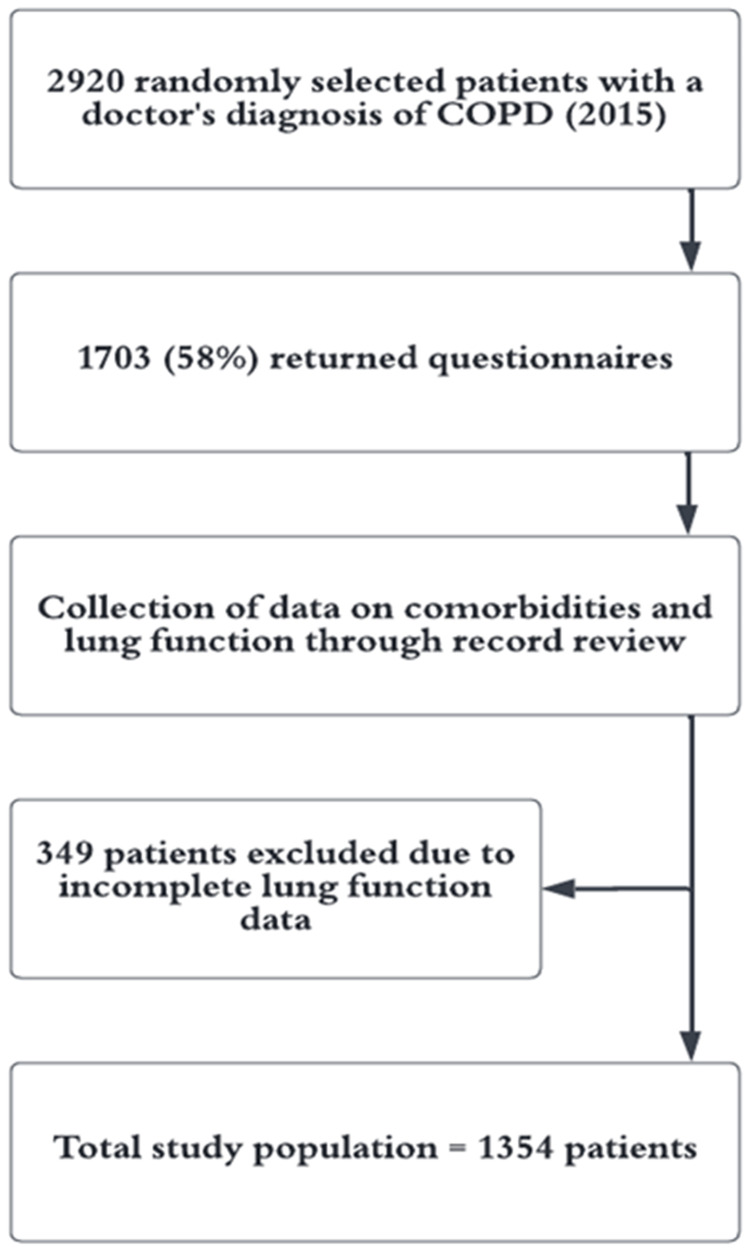
Methods: Cross-sectional analysis of 1354 patients from primary and secondary care, with a doctor's diagnosis of COPD. In 2014, data on demographics, exacerbation frequency and symptoms using COPD Assessment Test (CAT) were collected using questionnaires and on spirometry and comorbid conditions by record review. The non-exacerbator phenotype was defined as having reported no exacerbations the previous six months. Multivariable logistic regression with the non-exacerbator phenotype as dependent variable was performed, including stratification and interaction analyses by sex.
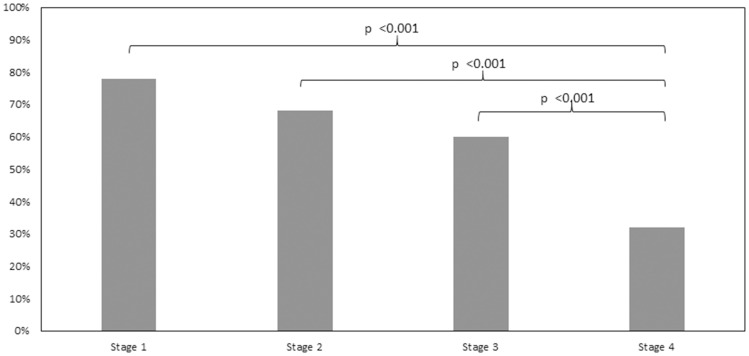
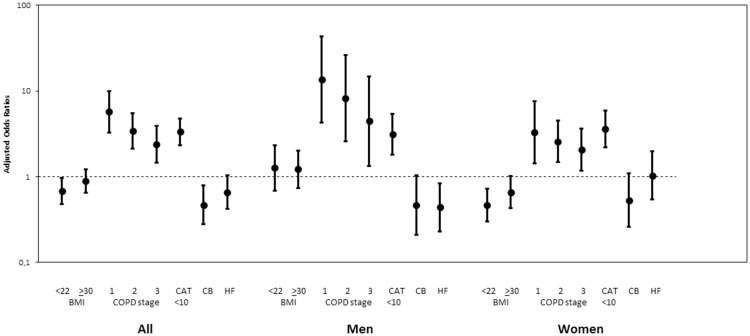
Results: The non-exacerbator phenotype was found in 891 (66%) patients and was independently associated with COPD stage 1 (OR [95% CI] 5.72 [3.30-9.92]), stage 2 (3.42 [2.13-5.51]) and stage 3 (2.38 [1.46-3.88]) compared with stage 4, and with CAT score <10 (3.35 [2.34-4.80]). Chronic bronchitis and underweight were inversely associated with the non-exacerbator phenotype (0.47 [0.28-0.79]) and (0.68 [0.48-0.97]), respectively. The proportion of non-exacerbators was higher among patients with no maintenance treatment or a single bronchodilator. The association of COPD stage 1 compared with stage 4 with the non-exacerbator phenotype was stronger in men (p for interaction 0.048). In women, underweight and obesity were both inversely associated with the non-exacerbator phenotype (p for interaction 0.033 and 0.046 respectively), and in men heart failure was inversely associated with the non-exacerbator phenotype (p for interaction 0.030).
Conclusion: The non-exacerbator phenotype is common, especially in patients with no maintenance treatment or a single bronchodilator, and is characterized by preserved lung function, low symptom burden, and by absence of chronic bronchitis, underweight and obesity and heart failure. We suggest these patients may need less treatment and follow-up, but that management of comorbid conditions is important to avoid exacerbations.
Keywords: CAT; COPD; body mass index; chronic bronchitis; exacerbations; heart failure; lung function; sex.
© 2023 Bouhuis et al.
Conflict of interest statement
Professor Christer Janson reports personal fees from AstraZeneca, Novartis, Boehringer Ingelheim, GlaxoSmithKline, Chiesi, Orion and Sanofi, outside the submitted work. Dr Karin Lisspers reports personal fees from Novartis, AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline, outside the submitted work. Dr Hanna Sandelowsky reports personal fees from Boehringer Ingelheim, Chiesi, Novartis, AstraZeneca, GlaxoSmithKline, and TEVA, outside the submitted work. Dr Björn Ställberg reports personal fees from AstraZeneca, Novartis, Boehringer Ingelheim, GlaxoSmithKleine, Meda/Mylan, Chiesi, and Teva, outside the submitted work. Dr Josefin Sundh reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi and Novartis, outside the submitted work. The authors report no other conflicts of interest related to this study.
Figures
Similar articles
-
Geographic variations of the prevalence and distribution of COPD phenotypes in Spain: "the ESPIRAL-ES study".Int J Chron Obstruct Pulmon Dis. 2018 Apr 10;13:1115-1124. doi: 10.2147/COPD.S158031. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29692606 Free PMC article.
-
COPD phenotypes: differences in survival.Int J Chron Obstruct Pulmon Dis. 2018 Jul 20;13:2245-2251. doi: 10.2147/COPD.S166163. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30050297 Free PMC article.
-
Distribution and characteristics of COPD phenotypes - results from the Polish sub-cohort of the POPE study.Int J Chron Obstruct Pulmon Dis. 2018 May 17;13:1613-1621. doi: 10.2147/COPD.S154716. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29844667 Free PMC article.
-
The characteristics of the frequent exacerbator with chronic bronchitis phenotype and non-exacerbator phenotype in patients with chronic obstructive pulmonary disease: a meta-analysis and system review.BMC Pulm Med. 2020 Apr 23;20(1):103. doi: 10.1186/s12890-020-1126-x. BMC Pulm Med. 2020. PMID: 32326924 Free PMC article.
-
The characteristics of the frequent exacerbators with chronic bronchitis phenotype and the asthma-chronic obstructive pulmonary disease overlap syndrome phenotype in chronic obstructive pulmonary disease patients: A meta-analysis and system review.Medicine (Baltimore). 2019 Nov;98(46):e17996. doi: 10.1097/MD.0000000000017996. Medicine (Baltimore). 2019. PMID: 31725666 Free PMC article.
Cited by
-
CRP, Fibrinogen, White Blood Cells, and Blood Cell Indices as Prognostic Biomarkers of Future COPD Exacerbation Frequency: The TIE Cohort Study.J Clin Med. 2024 Jun 30;13(13):3855. doi: 10.3390/jcm13133855. J Clin Med. 2024. PMID: 38999421 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
