

[Adrenal Vein Sampling in Primary Aldosteronism: A Pictorial Essay for Optimal Left-Side Sampling]
- PMID: 37051402
- PMCID: PMC10083640
- DOI: 10.3348/jksr.2021.0188
[Adrenal Vein Sampling in Primary Aldosteronism: A Pictorial Essay for Optimal Left-Side Sampling]
Abstract
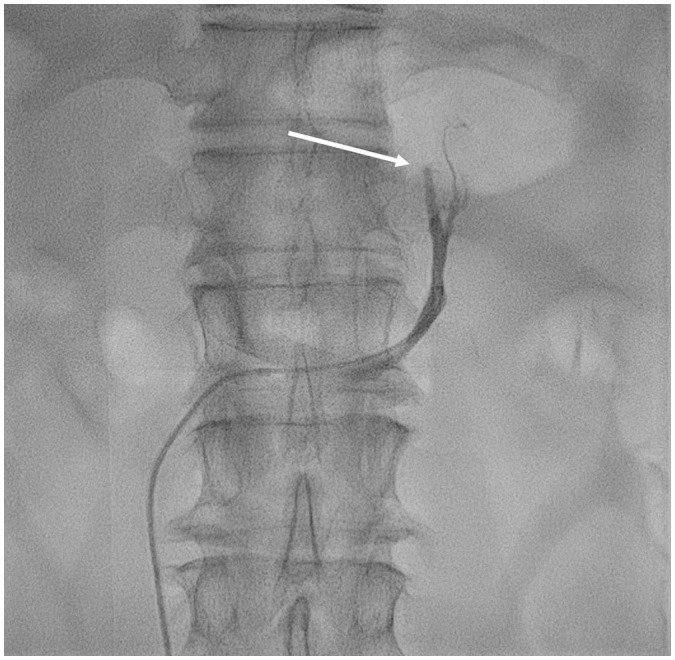
Primary aldosteronism (PA) is a curable cause of hypertension. Recent studies have revealed that the actual prevalence of PA is higher than previously recognized. Adrenal vein sampling (AVS) is an essential diagnostic procedure for revealing the cause of PA and determining the treatment plan. The success of AVS is confirmed by comparing cortisol levels between the samples from each adrenal vein and peripheral vein. The failure rate of the procedure is reported to be high in the right adrenal vein, which is directly connected to the inferior vena cava, while that in the left adrenal vein is relatively low; however, this has rarely been reported. In this review, we introduce and analyze cases of failure in left adrenal vein sampling.
일차성고알도스테론혈증의 원인을 감별하여 최종적인 치료방침을 결정하는 데 있어 필수적인 검사이다. 부신정맥채혈술의 성공 여부는 각 부신정맥에서 채혈한 샘플의 혈중 코티솔 농도와 말초혈관에서 채혈한 샘플의 혈중 코티솔 농도의 비를 측정하여 판단한다. 하대정맥으로 바로 연결되는 오른부신정맥에서 시술의 실패율이 더 높게 보고되며 상대적으로 왼부신정맥의 시술 실패율은 낮지만 드물게 보고된다. 본 임상화보에서는 왼부신정맥 부신정맥채혈술의 실패 사례를 소개하고 분석하여 최적의 부신정맥채혈술을 위한 고려사항에 대해 고찰하고자 한다.
Copyrights © 2023 The Korean Society of Radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
Figures





Similar articles
-
A single-centre experience of the implementation of adrenal vein sampling procedure: the impact on the diagnostic work-up in primary aldosteronism.Kardiol Pol. 2017;75(1):28-34. doi: 10.5603/KP.a2016.0166. Epub 2016 Nov 23. Kardiol Pol. 2017. PMID: 27878800
-
Comparison of Cortisol, Androstenedione and Metanephrines to Assess Selectivity and Lateralization of Adrenal Vein Sampling in Primary Aldosteronism.J Clin Med. 2021 Oct 17;10(20):4755. doi: 10.3390/jcm10204755. J Clin Med. 2021. PMID: 34682878 Free PMC article.
-
The Occurrence of Apparent Bilateral Aldosterone Suppression in Adrenal Vein Sampling for Primary Aldosteronism.J Endocr Soc. 2018 Mar 22;2(5):398-407. doi: 10.1210/js.2017-00481. eCollection 2018 May 1. J Endocr Soc. 2018. PMID: 29687091 Free PMC article.
-
Wide Variability in Catecholamine Levels From Adrenal Venous Sampling in Primary Aldosteronism.J Surg Res. 2022 Sep;277:1-6. doi: 10.1016/j.jss.2022.03.016. Epub 2022 Apr 19. J Surg Res. 2022. PMID: 35453052 Review.
-
Recent Advances in the Clinical Application of Adrenal Vein Sampling.Front Endocrinol (Lausanne). 2022 Feb 9;13:797021. doi: 10.3389/fendo.2022.797021. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35222268 Free PMC article. Review.
References
-
- Daunt N. Adrenal vein sampling: how to make it quick, easy, and successful. Radiographics. 2005;25 Suppl 1:S143–S158. - PubMed
-
- Baguet JP, Steichen O, Mounier-Véhier C, Gosse P. SFE/SFHTA/AFCE consensus on primary aldosteronism, part 1: epidemiology of PA, who should be screened for sporadic PA? Ann Endocrinol (Paris) 2016;77:187–191. - PubMed
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–2300. - PubMed
-
- Rossi GP, Seccia TM, Pessina AC. Primary aldosteronism - part I: prevalence, screening, and selection of cases for adrenal vein sampling. J Nephrol. 2008;21:447–454. - PubMed
-
- Scholten A, Cisco RM, Vriens MR, Shen WT, Duh QY. Variant adrenal venous anatomy in 546 laparoscopic adrenalectomies. JAMA Surg. 2013;148:378–383. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
