

Fibrinogen-to-prealbumin ratio: A new prognostic marker of resectable pancreatic cancer
- PMID: 37051547
- PMCID: PMC10083287
- DOI: 10.3389/fonc.2023.1149942
Fibrinogen-to-prealbumin ratio: A new prognostic marker of resectable pancreatic cancer
Abstract
Background: The fibrinogen-to-prealbumin ratio (FPR), a novel immune-nutritional biomarker, has been reported to be associated with prognosis in several types of cancer, but the role of FPR in the prognosis of resectable pancreatic cancer has not been elucidated.
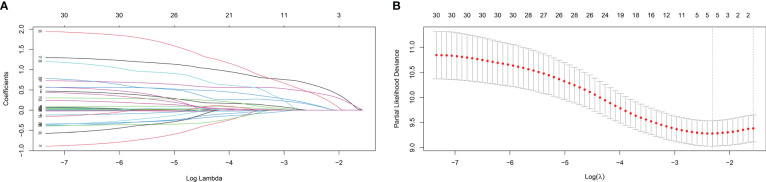
Methods: A total of 263 patients with resectable pancreatic cancer were enrolled in this study and were randomly divided into a training cohort (n = 146) and a validation cohort (n = 117). Receiver operating characteristic curve (ROC) was used to calculate the cut-off values of immune-nutritional markers. The least absolute shrinkage and selection operator (LASSO) regression and multivariate Cox regression were performed in the training cohort to identify the independent risk factors, based on which the nomogram was established. The performance of the nomogram was evaluated and validation by the training and validation cohort, respectively.
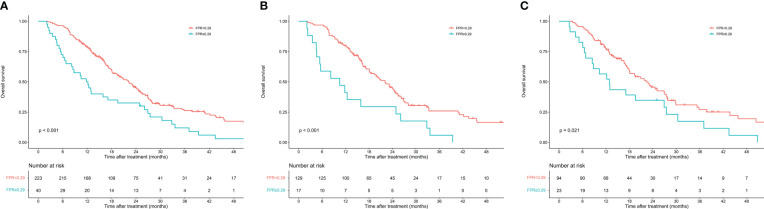
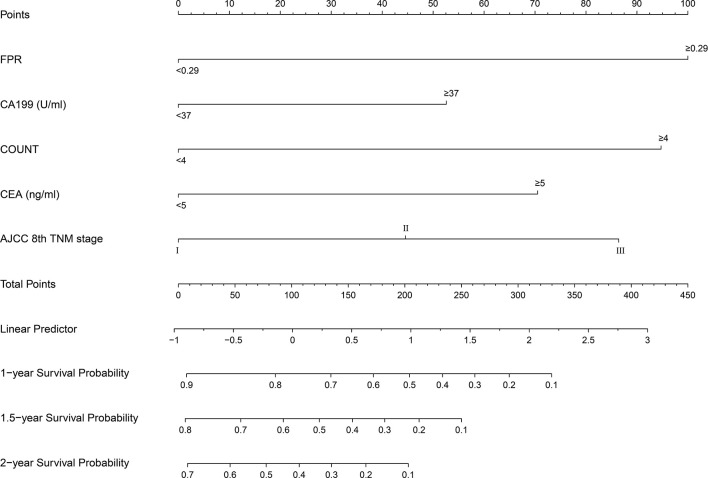
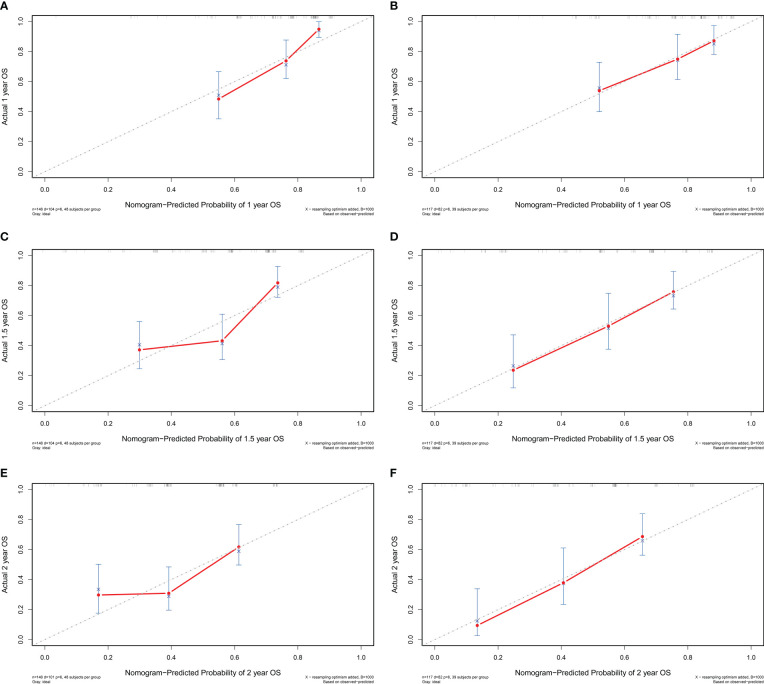
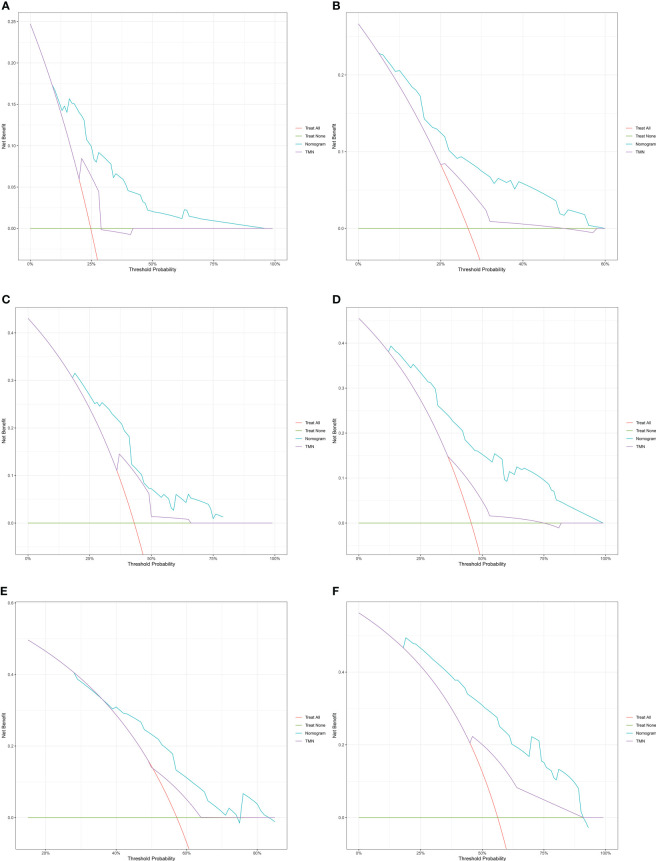
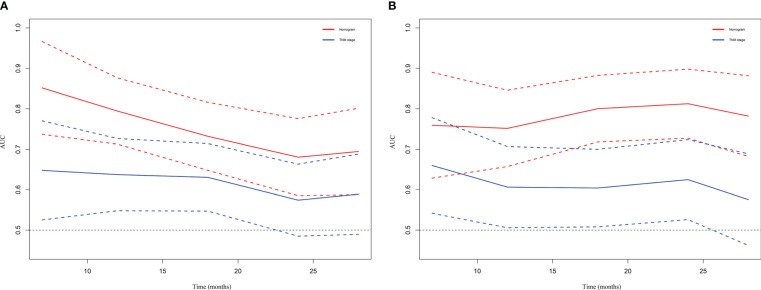
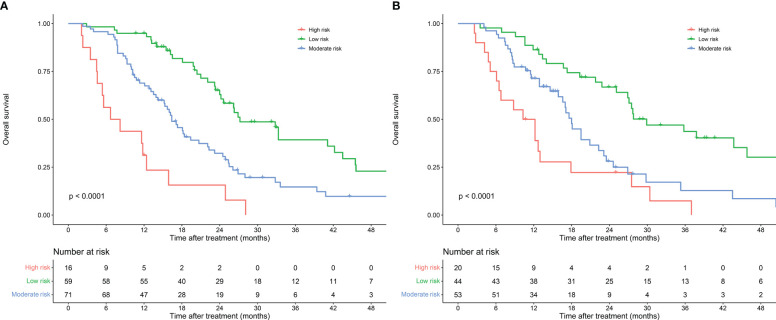
Results: The optimal cutoff value for FPR was 0.29. Multivariate analysis revealed that FPR, controlling nutritional status (CONUT), carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), and tumor node metastasis (TNM) stage were independent predictors of overall survival (OS). The nomogram was established by involving the five factors above. The C-index of the training cohort and validation cohort were 0.703 (95% CI: 0.0.646-0.761) and 0.728 (95% CI: 0.671-0.784). Decision curve analysis and time-dependent AUC showed that the nomogram had better predictive and discriminative ability than the conventional TNM stage.
Conclusion: FPR is a feasible biomarker for predicting prognosis in patients with resectable pancreatic cancer. The nomogram based on FPR is a useful tool for clinicians in making individualized treatment strategies and survival predictions.
Keywords: fibrinogen-to-prealbumin ratio; nomogram; prognosis; resectable pancreatic cancer; tumor marker.
Copyright © 2023 Li, Fan, Guo, Liang, Mao, Wu, Wang, Xu, Wu, Liu, Wang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Prognostic Value of Fibrinogen to Prealbumin Ratio (FPR) in Resectable Gastric Cancer.J Inflamm Res. 2024 Feb 27;17:1325-1335. doi: 10.2147/JIR.S440832. eCollection 2024. J Inflamm Res. 2024. PMID: 38434582 Free PMC article.
-
The prognostic value of preoperative fibrinogen-to-prealbumin ratio and a novel FFC score in patients with resectable gastric cancer.BMC Cancer. 2020 May 6;20(1):382. doi: 10.1186/s12885-020-06866-6. BMC Cancer. 2020. PMID: 32375697 Free PMC article.
-
Development and Validation of a Nomogram Based on Nutritional Indicators and Tumor Markers for Prognosis Prediction of Pancreatic Ductal Adenocarcinoma.Front Oncol. 2021 May 31;11:682969. doi: 10.3389/fonc.2021.682969. eCollection 2021. Front Oncol. 2021. PMID: 34136406 Free PMC article.
-
Value of the fibrinogen-platelet ratio in patients with resectable pancreatic cancer.J Med Invest. 2021;68(3.4):342-346. doi: 10.2152/jmi.68.342. J Med Invest. 2021. PMID: 34759156
-
A NOVEL PROGNOSTIC INDEX IN PATIENTS WITH RESECTABLE ESOPHAGEAL SQUAMOUS CELL CARCINOMA: FIBRINOGEN/PREALBUMIN RATIO.Rev Invest Clin. 2020;72(1):46-54. doi: 10.24875/RIC.19003184. Rev Invest Clin. 2020. PMID: 32132740
Cited by
-
Prognostic Assessment of Colorectal Cancer Patients after Laparoscopic Surgery: A Comprehensive Evaluation of the Glasgow Prognostic Score and Fibrinogen-to-Prealbumin Ratio.Med Sci Monit. 2024 Feb 21;30:e942658. doi: 10.12659/MSM.942658. Med Sci Monit. 2024. PMID: 38379279 Free PMC article.
-
Low prealbumin level is a poor prognostic biomarker for surgically treated pancreatic cancer.Mol Clin Oncol. 2025 Apr 30;23(1):61. doi: 10.3892/mco.2025.2856. eCollection 2025 Jul. Mol Clin Oncol. 2025. PMID: 40370692 Free PMC article.
-
Prognostic role of fibrinogen-to-albumin ratio in patients with gynecological cancers: a meta-analysis.Front Oncol. 2025 Jul 3;15:1580940. doi: 10.3389/fonc.2025.1580940. eCollection 2025. Front Oncol. 2025. PMID: 40678069 Free PMC article.
-
Fibrinogen to pre-albumin ratio is an independent prognostic index for patients with pancreatic ductal adenocarcinoma after radical resection.World J Surg Oncol. 2024 Oct 28;22(1):284. doi: 10.1186/s12957-024-03524-0. World J Surg Oncol. 2024. PMID: 39468569 Free PMC article.
-
Prognostic value of peripheral blood fibrinogen-to-albumin ratio and neutrophil-to-lymphocyte ratio in patients with locally advanced or metastatic pancreatic cancer.Am J Transl Res. 2024 Nov 15;16(11):7165-7175. doi: 10.62347/ZOHP7650. eCollection 2024. Am J Transl Res. 2024. PMID: 39678563 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials