

Incorporation of the 40-Gene Expression Profile (40-GEP) Test to Improve Treatment Decisions in High-Risk Cutaneous Squamous Cell Carcinoma (cSCC) Patients: Case Series and Algorithm
- PMID: 37051586
- PMCID: PMC10083143
- DOI: 10.2147/CCID.S403330
Incorporation of the 40-Gene Expression Profile (40-GEP) Test to Improve Treatment Decisions in High-Risk Cutaneous Squamous Cell Carcinoma (cSCC) Patients: Case Series and Algorithm
Abstract
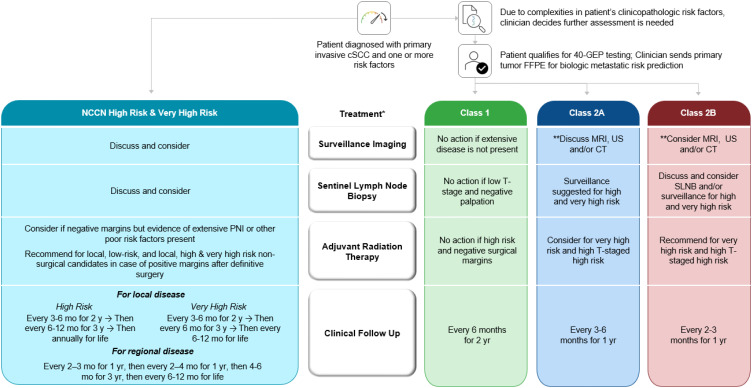
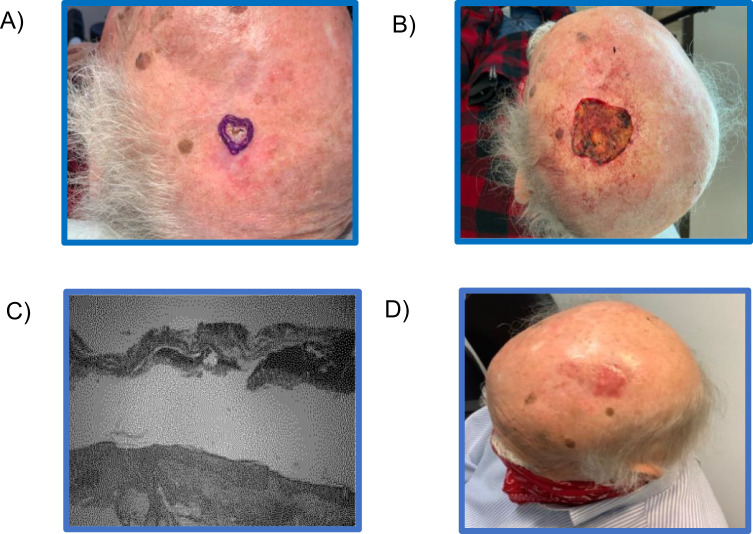
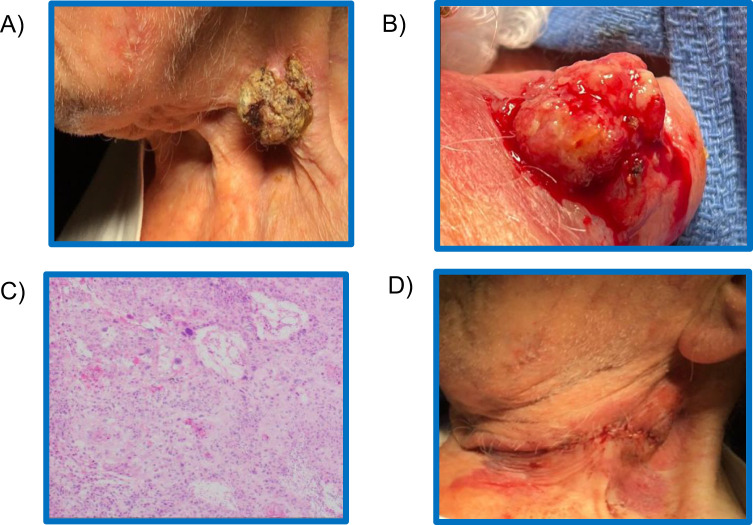
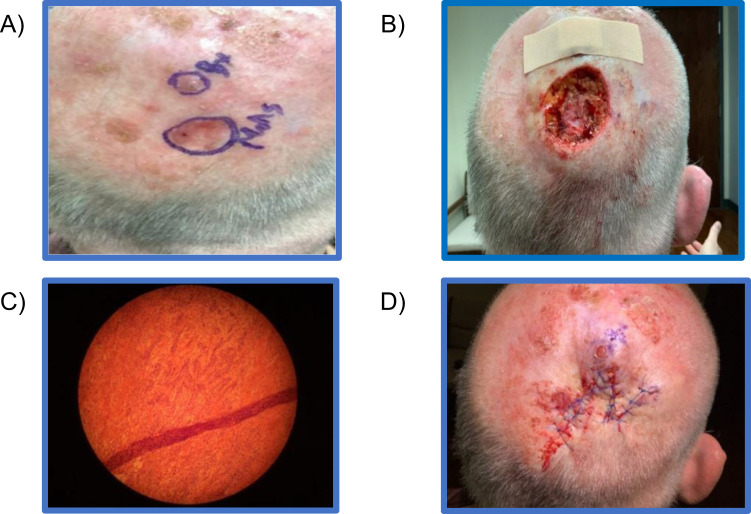
Cutaneous squamous cell carcinoma (cSCC) has become a significant public health issue due to its rapidly rising incidence and an estimated 1.8 million newly diagnosed cases annually. As with other cancers, treatment decisions for patients with cSCC are based primarily on a patient's risk for poor outcomes. There has been improvement in clinicopathologic factor-based risk assessment approaches, either through informal methods or ever evolving staging approaches. However, these approaches misidentify patients who will eventually have disease progression as low-risk and conversely, over classify patients as high-risk who do not experience relapse. To improve the accuracy of risk assessment for patients with cSCC, the 40-gene expression profile (40-GEP) test has been validated to show statistically significant stratification of a high-risk cSCC patient's risk of nodal or distant metastasis, independent of currently available risk-assessment methods. The 40-GEP test allows for a more accurate classification of metastatic risk for high-risk cSCC patients, with the aim to influence appropriate allocation of clinician time and therapeutic resources to those patients who will most benefit. The objective of this article is to present a treatment algorithm in which clinicians can easily integrate the results of the 40-GEP test into their current treatment approaches to tailor patient care based on individual tumor biology. The following modalities were considered: surveillance imaging, sentinel lymph node biopsy (SLNB), adjuvant radiation therapy (ART), and clinical follow-up. The authors have contributed their own cases for discussion as to how they have seen the beneficial impact of 40-GEP test results in their own practice. Overall, clinicians can identify risk-aligned treatment pathway improvements with the use of the 40-GEP test for challenging to manage, high-risk cSCC patients.
Keywords: 40-GEP; 40-gene expression profile; cSCC; clinician algorithm; cutaneous squamous cell carcinoma; metastasis; patient management; prognostic; risk-stratification.
© 2023 Singh et al.
Conflict of interest statement
GS is a consultant for Castle Biosciences Inc., during the conduct of the study and a consultant for Regeneron, outside the submitted work. ASF is an advisor for Castle Biosciences Inc. and Regeneron. SNT declares no relevant conflicts of interest in this work. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
Similar articles
-
Integrating 40-GEP Testing to Improve Clinical Recommendations for Adjuvant Radiation for Cutaneous Squamous Cell Carcinoma: Multidisciplinary Consensus Guidelines.J Clin Aesthet Dermatol. 2024 Mar;17(3 Suppl 2):S3-S8. J Clin Aesthet Dermatol. 2024. PMID: 38495846 Free PMC article. Review.
-
Clinical Utility of the 40-Gene Expression Profile (40-GEP) Test for Improved Patient Management Decisions and Disease-Related Outcomes when Combined with Current Clinicopathological Risk Factors for Cutaneous Squamous Cell Carcinoma (cSCC): Case Series.Dermatol Ther (Heidelb). 2022 Feb;12(2):591-597. doi: 10.1007/s13555-021-00665-y. Epub 2021 Dec 23. Dermatol Ther (Heidelb). 2022. PMID: 34951694 Free PMC article.
-
Gene expression profiling for metastatic risk in head and neck cutaneous squamous cell carcinoma.Laryngoscope Investig Otolaryngol. 2022 Jan 6;7(1):135-144. doi: 10.1002/lio2.724. eCollection 2022 Feb. Laryngoscope Investig Otolaryngol. 2022. PMID: 35155791 Free PMC article.
-
Real-World Evidence Shows Clinicians Appropriately Use the Prognostic 40-Gene Expression Profile (40-GEP) Test for High-Risk Cutaneous Squamous Cell Carcinoma (cSCC) Patients.Cancer Invest. 2022 Nov;40(10):911-922. doi: 10.1080/07357907.2022.2116454. Epub 2022 Sep 15. Cancer Invest. 2022. PMID: 36073945
-
The Prognostic Value and Clinical Utility of the 40-Gene Expression Profile (40-GEP) Test in Cutaneous Squamous Cell Carcinoma: Systematic Review and Meta-Analysis.Cancers (Basel). 2023 Apr 25;15(9):2456. doi: 10.3390/cancers15092456. Cancers (Basel). 2023. PMID: 37173922 Free PMC article. Review.
Cited by
-
40-Gene expression profile test predicting metastatic risk in localized, high-risk cutaneous squamous cell carcinoma for peer review.SAGE Open Med Case Rep. 2024 Sep 25;12:2050313X241284141. doi: 10.1177/2050313X241284141. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 39328268 Free PMC article.
-
Integrating the 40-Gene Expression Profile (40-GEP) Test Improves Metastatic Risk-Stratification Within Clinically Relevant Subgroups of High-Risk Cutaneous Squamous Cell Carcinoma (cSCC) Patients.Dermatol Ther (Heidelb). 2024 Mar;14(3):593-612. doi: 10.1007/s13555-024-01111-5. Epub 2024 Mar 1. Dermatol Ther (Heidelb). 2024. PMID: 38424384 Free PMC article.
-
The Role of Gene Expression Profiling in the Management of Cutaneous Squamous Cell Cancer: A Review.Cancers (Basel). 2024 Nov 23;16(23):3925. doi: 10.3390/cancers16233925. Cancers (Basel). 2024. PMID: 39682114 Free PMC article. Review.
-
Integrating 40-GEP Testing to Improve Clinical Recommendations for Adjuvant Radiation for Cutaneous Squamous Cell Carcinoma: Multidisciplinary Consensus Guidelines.J Clin Aesthet Dermatol. 2024 Mar;17(3 Suppl 2):S3-S8. J Clin Aesthet Dermatol. 2024. PMID: 38495846 Free PMC article. Review.
-
Use of the 40-gene Expression Profile (40-GEP) Test in Medicare-eligible Patients Diagnosed with Cutaneous Squamous Cell Carcinoma (cSCC) to Guide Adjuvant Radiation Therapy (ART) Decisions Leads to a Significant Reduction in Healthcare Costs.J Clin Aesthet Dermatol. 2024 Jan;17(1):41-44. J Clin Aesthet Dermatol. 2024. PMID: 38298751 Free PMC article.
References
-
- Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer (Keratinocyte carcinomas) in the US Population, 2012. JAMA Dermatol. 2015;151:1081–1086. - PubMed
-
- Schmults CD, Karia PS, Carter JB, et al. Factors predictive of recurrence and death from cutaneous squamous cell carcinoma: a 10-year, single-institution cohort study. JAMA Dermatol. 2013;149:541–547. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
