A Preliminary Experience of Endoscopic Total Mastectomy With Immediate Free Abdominal-Based Perforator Flap Reconstruction Using Minimal Incisions, and Literature Review
- PMID: 37051645
- PMCID: PMC10139846
- DOI: 10.4048/jbc.2023.26.e10
A Preliminary Experience of Endoscopic Total Mastectomy With Immediate Free Abdominal-Based Perforator Flap Reconstruction Using Minimal Incisions, and Literature Review
Abstract
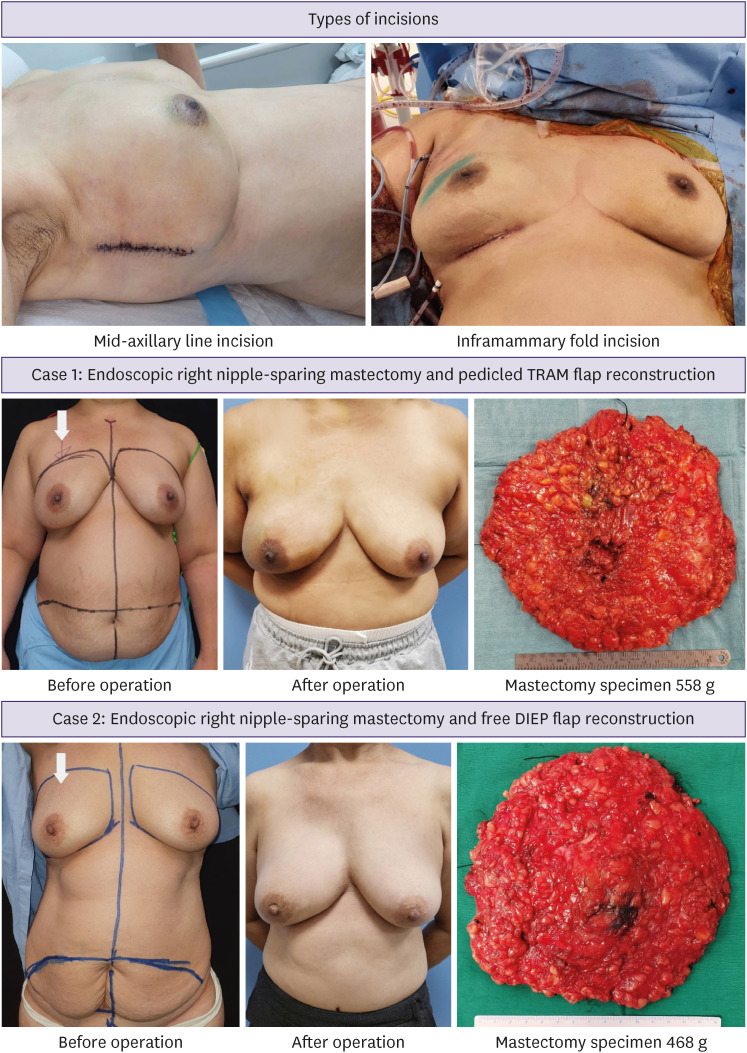
Purpose: Endoscopic total mastectomy (ETM) is predominantly performed with reconstruction using prostheses, lipofilling, omental flaps, latissimus dorsi flaps, or a combination of these techniques. Common approaches include minimal incisions, e.g., periareolar, inframammary, axillary, or mid-axillary line, which limit the technical ability to perform autologous flap insets and microvascular anastomoses, as such the ETM with free abdominal-based perforator flap reconstruction has not been robustly explored.
Methods: We studied female patients with breast cancer who underwent ETM and abdominal-based flap reconstruction. Clinical-radiological-pathological characteristics, surgery, complications, recurrence rates, and aesthetic outcomes were reviewed.
Results: Twelve patients underwent ETM with abdominal-based flap reconstruction. The mean age was 53.4 years (range 36-65). Of the patients, 33.3% were surgically treated for stage I, 58.4% for stage II, and 8.3% for stage III cancer. Mean tumor size was 35.4 mm (range 1-67). Mean specimen weight was 458.75 g (range 242-800). Of the patients, 92.3% successfully received endoscopic nipple-sparing mastectomy and 7.7% underwent intraoperative conversion to skin-sparing mastectomy after carcinoma was reported on frozen section of the nipple base. Mean operative time for ETM was 139 minutes (92-198), and the average ischemic time was 37.3 minutes (range 22-50). Fifty percent of patients underwent deep inferior epigastric perforator, 33.4% underwent MS-2 transverse rectus abdominis musculocutaneous (TRAM), 8.3% underwent MS-1 TRAM, and 8.3% underwent pedicled TRAM flap reconstruction. No cases required re-exploration, no flap failure occurred, margins were clear, and no skin or nipple-areolar complex ischemia/necrosis developed. In the aesthetic outcome evaluation, 16.7% were excellent, 75% good, 8.3% fair, and none were unsatisfactory. No recurrences were observed.
Conclusion: ETM through a minimal-access inferior mammary or mid-axillary line approach, followed by immediate pedicled TRAM or free abdominal-based perforator flap reconstruction, can be a safe means of achieving an "aesthetically scarless" mastectomy and reconstruction through minimal incisions.
Keywords: Breast Neoplasms; Free Tissue Flap; Mastectomy, Subcutaneous; Perforator Flap.
© 2023 Korean Breast Cancer Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tamaki Y, Sakita I, Miyoshi Y, Sekimoto M, Takiguchi S, Monden M, et al. Transareolar endoscopy-assisted partial mastectomy: a preliminary report of six cases. Surg Laparosc Endosc Percutan Tech. 2001;11:356–362. - PubMed
-
- Nakajima H, Sakaguchi K, Mizuta N, Hachimine T, Ohe S, Sawai K. Video-assisted total glandectomy and immediate reconstruction for breast cancer. Biomed Pharmacother. 2002;56(Suppl 1):205s–208s. - PubMed
LinkOut - more resources
Full Text Sources