Hungry runners - low energy availability in male endurance athletes and its impact on performance and testosterone: mini-review
- PMID: 37052052
- PMCID: PMC10388605
- DOI: 10.4081/ejtm.2023.11104
Hungry runners - low energy availability in male endurance athletes and its impact on performance and testosterone: mini-review
Erratum in
-
Correction. Hungry runners - low energy availability in male endurance athletes and its impact on performance and testosterone: mini-review.Eur J Transl Myol. 2025 Jun 27;35(2):13900. doi: 10.4081/ejtm.2025.13900. Epub 2025 Apr 16. Eur J Transl Myol. 2025. PMID: 40237160 Free PMC article.
Abstract
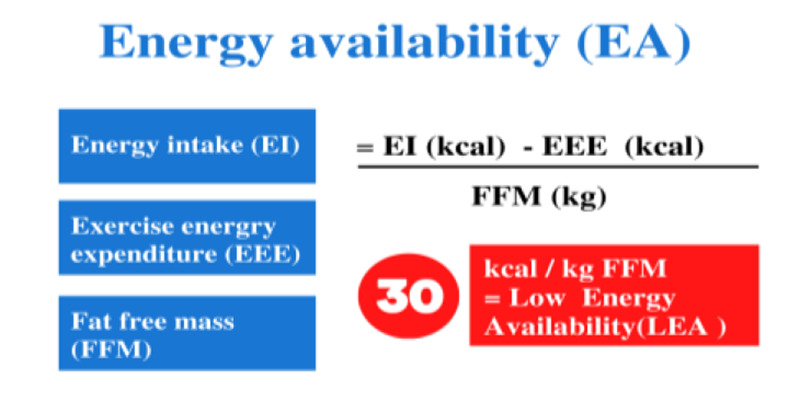
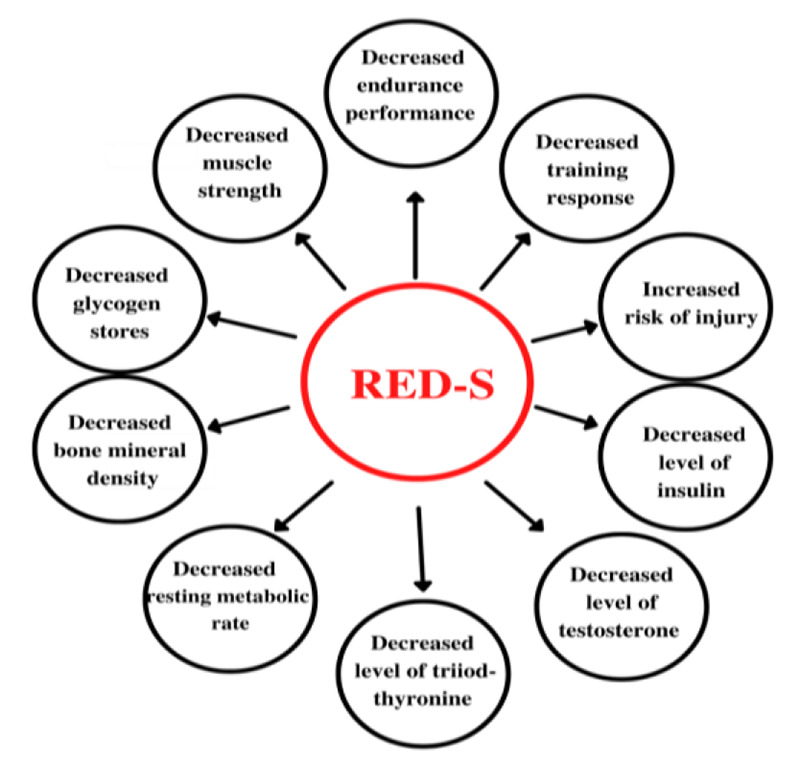
Low Energy Availability (LEA) arises from the inability to cover energy needs and requirements of training or normal physiological functions. This value differs from the energy balance, which takes into account the total daily energy intake compared to all the energy expended, regardless of the amount of fat-free mass. Insufficient energy consumption affects recovery, adaptation processes, increases the risk of injury or illness, so all of this can negatively affect performance. This mini-review is written on research articles in Pubmed database related to LEA in endurance-trained men and its impact on performance and testosterone. This article also clarifies the prevalence of LEA in male endurance athletes and its correlation to Relative Energy Deficiency in Sports (RED-S). LEA occurs in male endurance athletes and correlates with decreased testosterone levels, decreased bone density and also Resting Metabolic Rate. In endurance-trained men, there is great potential for the negative consequences of low energy availability. It can also be said that there are possibilities for primary screening, so we recommend regular check-ups of blood markers, body structure and keeping not only training but also dietary records, which can increase awareness of an adequate energy balance.
Conflict of interest statement
Prevalence of LEA
Chronic low energy intake can stem from a variety of reasons: i) lack of knowledge about proper nutrition and nutritional sources to achieve energy balance, ii) lack of time to prepare meals, iii) lack of skills in preparing meals, iv) financial reasons, or v) physiological reasons like loss of appetite after training due to suppression of ghrelin production. In these cases, it is not necessarily a matter of intentionally regulating energy income. In general, it does not matter whether it is an intentional or unintentional restriction of energy income. The consequences are identical in both cases. In the case of intentional control or restriction of energy intake, the most common reasons are dissatisfaction with your body and the desire to change body composition. While most LEA and body image studies have focused primarily on women, on the other hand, there is growing evidence that problems with body image and eating habits are also common in male athletes - as we would like to describe in this minireview. Investigations among sport types demonstrated that athletes who participate in sports emphasizing leanness, including endurance sports (cycling and running), appear to have a greater prevalence of Disordered Eating (DE). Among a sample male cyclists and male non-cyclists, cyclists exhibited a significantly higher overall score on the Eating Attitudes Test (EAT)-26 (indicating more DE), and a higher score on the dieting and binge eating EAT-26 sub-factors. In the largest epidemiological study to date which evaluated the prevalence of Eating Disorders (EDs) elite Norwegian male athletes (n=687) and non-athlete controls (n=629) were studied. Results reported an 8 % prevalence of EDs, including anorexia nervosa, bulimia nervosa, ED not otherwise specified, and anorexia athletica, among the 687 male athletes compared with a 0.5 % prevalence among the 629 male non-athlete controls. Ferrand and Brunet (2004) evaluated a sample of 42 elite male cyclists and found that over 57% had an EAT-26 score. Among a sample of male cyclists, Filaire et al. (2007) found that 67% were not satisfied with their weight, 41% dieted to lose weight, and others reported laxative use and increased exercise for weight-control purposes. Three investigations in male runners and cyclists identified low caloric intake in athletes, although food and fluid intake surrounding and during competition largely met recommended levels in most reports.(21-23) Similar to weight class and aesthetic sports, several studies have identified similar deficits in male endurance athletes. One report evaluating 37 male adolescent cyclists and controls found that, despite cyclists exercising fivefold more hours per week than controls, their energy intake (2300 kcal/day) did not significantly exceed that of control subjects and appeared to fall below recommended intake levels based on their level of training. Additionally, intake of calcium, vitamin D, iron, and B vitamins were below recommendations for both cyclists and controls. As we could see in the previous chapter LEA is a widespread phenomenon across several sports for both men and women. It seems that there is a lower risk of low EA in team sports and ball games. Studies investigating EA among male adolescent athletes competing in ball or team sports, such as football, soccer, and ice hockey, indicate sufficient absolute (kcal) and relative (kcal/kg) energy intake, ranging from 40 to 60 kcal/kg FFM.(24,25) In this minireview, we focused on the prevalence of low energy availability of endurance-trained men. Details are given in Table 1 below. The concept of adequate energy availability has not been sufficiently studied in male athletes. Despite the fact that women can be considered risky in terms of the consequences of LEA, for men, LEA, hypogonadism and bone health are three interconnected components. An electronic database of “Pubmed” was chosen to search for relevant studies. This also included backward search according to the references in the included articles. The keywords "energy availability, endurance, testosterone, male hypogonadism, sports performance, hormones" were used to search for relevant resources. The main selection criterion was that the studies had to deal with low energy availability in endurance-trained men. Furthermore, there was a requirement for a publication date between 2017-2022 and the availability of full-text.
Hypogonadism and testosterone disturbances
The Endocrine Society defines male hypogonadism as a clinical syndrome resulting from the failure of the testis to produce physiological levels of testosterone (androgen deficiency) and a normal number of spermatozoa. Hypogonadism (primary, secondary or mixed) is caused by disruption of one or more levels of the hypothalamic–pituitary–gonadal axis. Boloña et al. (2007) claim that testosterone is associated with various processes in the male organism including androgenic-anabolic it is thought, but not universally accepted that it is a crucial factor for male sexual libido. As has been noted, the definition of hypogonadism in medicine differs from the ambiguous definition in the field of sports, where it can be a functional condition and, importantly, this condition is relatively quickly reversible to a normal condition.(29-31) The prevalence of exercise-associated hypogonadotropic hypogonadism and its impact on skeletal health in male athletes is not well understood. This is partly due to the lack of research on this topic and also because the identification of hypogonadism in men is not as clear as in women, where the situation is facilitated by the so-called menstrual dysfunction. In some cases, decreased testosterone levels may still be within the clinically normal range and may be considered an exercise-induced functional state. In terms of sports performance, testosterone provides physiological benefits such as increased muscle development, increased erythropoiesis, increased hemoglobin levels, which facilitate the transfer of oxygen in the blood and, last but not least, increased aerobic capacity. There are pioneering studies in animal models where has been shown that food deprivation suppresses spermatogenesis. If negative energy balance is associated with disturbances in reproductive function in male runners remains speculative but very likely.(33,34) De Souza (2021) assumes that alterations in testosterone concentration and spermatogenesis are an initial physiological adaptation caused by insufficient energy intake. When there is a state of chronic negative energy balance, reproductive function might be suppressed in order to prevent energy loss. Further evidence suggests that endurance-exercising males can develop a similar suppression of the reproductive function which we know from women. It is called Exercise Hypogonadal Male Condition (EHMC). EHMC can be viewed as overreaching or overtraining, when the amount of training was not adequately balanced by rest, resulting in physiological or psychological symptoms of maladaptation. Despite the obvious similarities between EHMC, overtraining, the women's athletic triad and RED-S, the differences should be put into perspective. The European College of Sport Science and the American College of Sports Medicine agree that when overreaching or overtraining is suspected, it is important to rule out other hypothetical causes related to negative energy balance or low energy availability. If the cause of the symptoms is an energy deficit, we do not classify this situation in the area of overreaching or overtraining, but it falls under RED-S. Being more physically active has been shown to be beneficial reproductively for men who are sedentary (or have a very low physical activity levels) as it results in improved testosterone levels and libido. Conversely, there are many reports suggesting that men who participate in large amounts of endurance exercise training (
Energy availability and endurance performance in males
The overall amount of research examining endocrine dysfunctions due to low EA in men is only limited compared to research in women. The most evidence is provided by research into the effect of LEA on the reproductive abilities of men, which we mentioned in the previous text. Ultra-endurance exercise can cause acute decreases in testosterone levels as well as increases in cortisol, suggesting significant suppression of hypothalamic-pituitary axis functions. Cortisol as one of the markers of endocrine stress is often associated with reduced testosterone circulation. This was seen in male endurance athletes who were exposed to low EA. It was also observed that a higher short-term energy deficit (24 hours) was associated with higher cortisol levels in performance endurance athletes compared to their counterparts with sufficient EA. A study of elite rowers who underwent a four-week intensive training block with reduced energy supply found worsened regeneration and worsened performance on a 5,000-meter track. Decreased aerobic and anaerobic performance, weight loss, and reduced RMR have also been shown in trained cyclists with insufficient energy intake during the intense training period. In male cyclists, long-term low EA at the current higher training load resulted in reduced performance, and no benefit in terms of performance was found due to the amount of body fat. Regarding the effect on muscle proteins, we know that the stimulation of muscle protein synthesis is supported by anabolic hormones such as insulin and testosterone. On the other hand, glucocorticoids, such as cortisol, increase the turnover of proteins in the body and initiate the breakdown of skeletal muscle proteins. As described by Šarabon et al., (2022), muscle strength and especially eccentric load is important for runners. The effect of low EA on performance may be more difficult to identify due to the significant effect of lower body weight on performance, thus even leading to a relative improvement in performance. Disease-related training failure is shown to be three times higher in athletes at low EA risk. These athletes lose more than 22 days of training per year, with an average of 7 days for risk-free athletes. When evaluating the association between endurance training and sexual libido in men, it has been shown that libido scores are related to the duration and intensity of training, and thus the ability to train longer or harder. Athletes usually follow a strict regimen and a hard training regimen to optimize athletic performance. In this endeavor, athletes may be malnourished enough to enter a state of low energy availability due to consuming too little energy compared to overpowering over a long period of time. This can have devastating effects, including damage to multiple organ systems, lower Bone Mineral Density (BMD), decreased testosterone levels, increased risk of injury, impaired coordination, and decreased athletic performance in many ways.(54,45,50,55)
Final considerations
The LEA seems to be a significant factor affecting the hormonal system and sports performance of endurance trained men. There is a fine line between the benefits of lower body weight and the negative consequences of LEA. This is linked with insufficient testosterone production, reduced libido, decreased bone mineral density. As we can see, the problem of low energy availability is better documented in women and on the contrary understudied in men. Its manifestations in men are more difficult to detect, and that is why we perceive a high need to include screening for nutritional risks as part of regular check-ups with a sports or physical education doctor. At the same time, we dare to say that there is a need for an easily accessible screening tool that can also be used outside of laboratory conditions. The athlete himself may see this as sudden weight changes, performance stagnation, fatigue fractures and digestive problems. It will be crucial for further research to reveal the relationships between a particular level of energy availability per organism - not just during the exercise itself and especially in the long term. More research is also needed for assessing long-term effects of LEA that result from various periods of sports training during the season.
Figures
References
-
- Sundgot-Borgen J, Torstveit MK. Aspects of disordered eating continuum in elite high-intensity sports. Scand J Med Sci Sports. 2010. Oct;20 Suppl 2:112-21. doi: 10.1111/j.1600-0838.2010.01190.x. PMID: 20840569. - PubMed
-
- Slater J, Brown R, McLay-Cooke R, Black K. Low Energy Availability in Exercising Women: Historical Perspectives and Future Directions. Sports Med. 2017. Feb;47(2):207-220. doi: 10.1007/s40279-016-0583-0. PMID: 27430502. - PubMed
-
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, Lebrun C, Lundy B, Melin AK, Meyer NL, Sherman RT, Tenforde AS, Klungland Torstveit M, Budgett R. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. 2018. Jun;52(11):687-697. doi: 10.1136/bjsports-2018-099193. PMID: 29773536. - PubMed
-
- De Souza MJ, Koltun KJ., Williams NI. What is the evidence for a Triad-like syndrome in exercising men? Current Opinion in Physiology. 2019. Apr; 10. doi:10.1016/j.cophys.2019.04.002
-
- Nattiv A, De Souza MJ, Koltun KJ, Misra M, Kussman A, Williams NI, Barrack MT, Kraus E, Joy E, Fredericson M. The Male Athlete Triad-A Consensus Statement From the Female and Male Athlete Triad Coalition Part 1: Definition and Scientific Basis. Clin J Sport Med. 2021. Jul 1;31(4):345-353. doi 10.1097/JSM.0000000000000946. PMID: 34091537. - PubMed
LinkOut - more resources
Full Text Sources