

Buspirone for early satiety and symptoms of gastroparesis: A multi-centre, randomised, placebo-controlled, double-masked trial (BESST)
- PMID: 37052334
- PMCID: PMC10202558
- DOI: 10.1111/apt.17479
Buspirone for early satiety and symptoms of gastroparesis: A multi-centre, randomised, placebo-controlled, double-masked trial (BESST)
Abstract
Background: Patients with gastroparesis and related disorders have symptoms including early satiety, postprandial fullness and bloating. Buspirone, a 5-HT1 receptor agonist, may improve fundic accommodation.
Aim: To determine if buspirone treatment improves early satiety and postprandial fullness in patients with symptoms of gastroparesis.
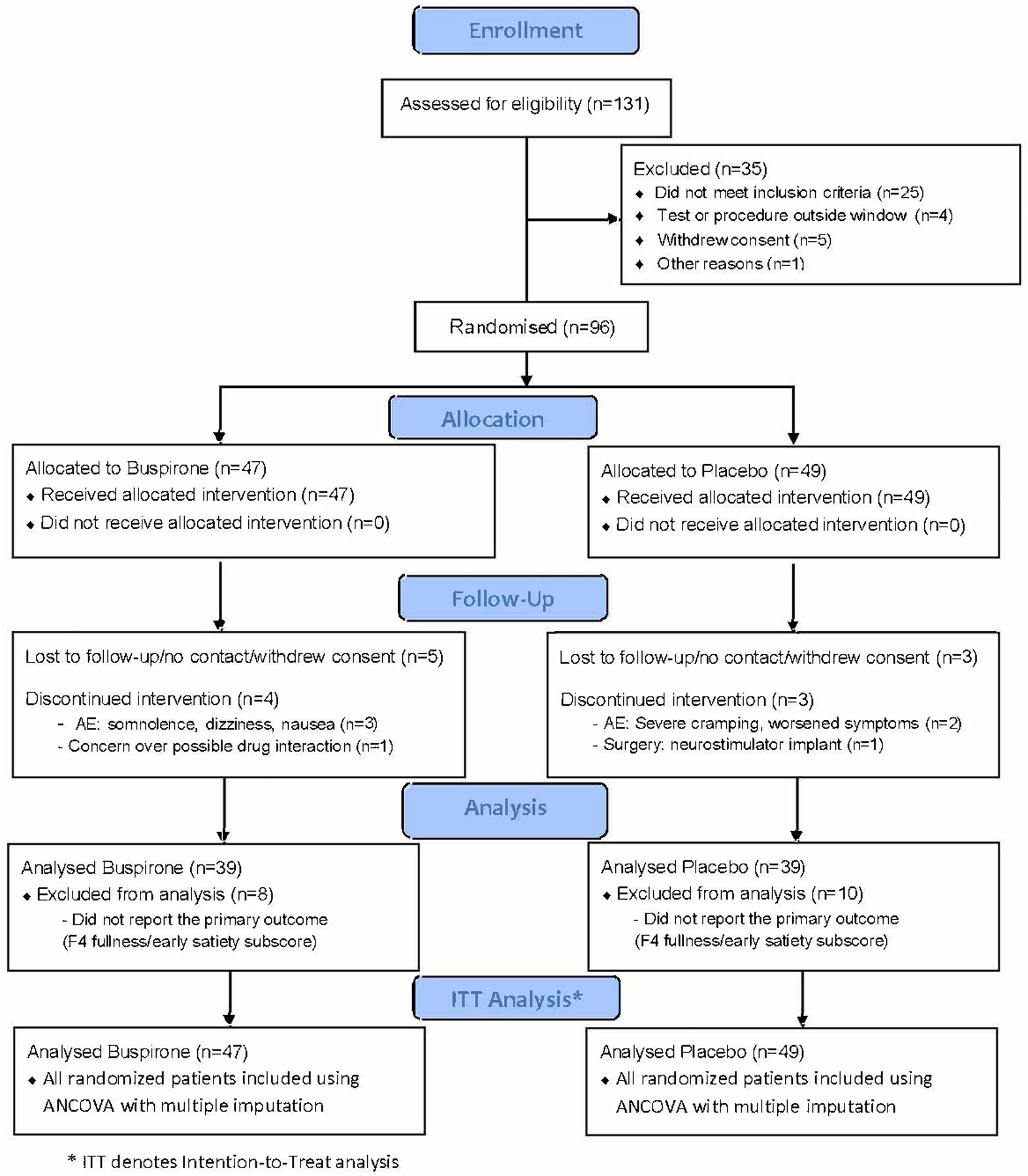
Methods: This 4-week multi-centre clinical trial randomised patients with symptoms of gastroparesis and moderate-to-severe symptoms of fullness (Gastroparesis Cardinal Symptom Index [GCSI] early satiety/postprandial fullness subscore [ES/PPF]) to buspirone (10 mg orally) or placebo three times per day. The primary outcome was a change in the ES/PPF from baseline to 4 weeks. The primary analysis was per protocol intention-to-treat ANCOVA of between-group baseline vs. 4-week differences (DoD) in ES/PPF adjusted for baseline ES/PPF. Results are reported using both nominal and Bonferroni (BF) p values.
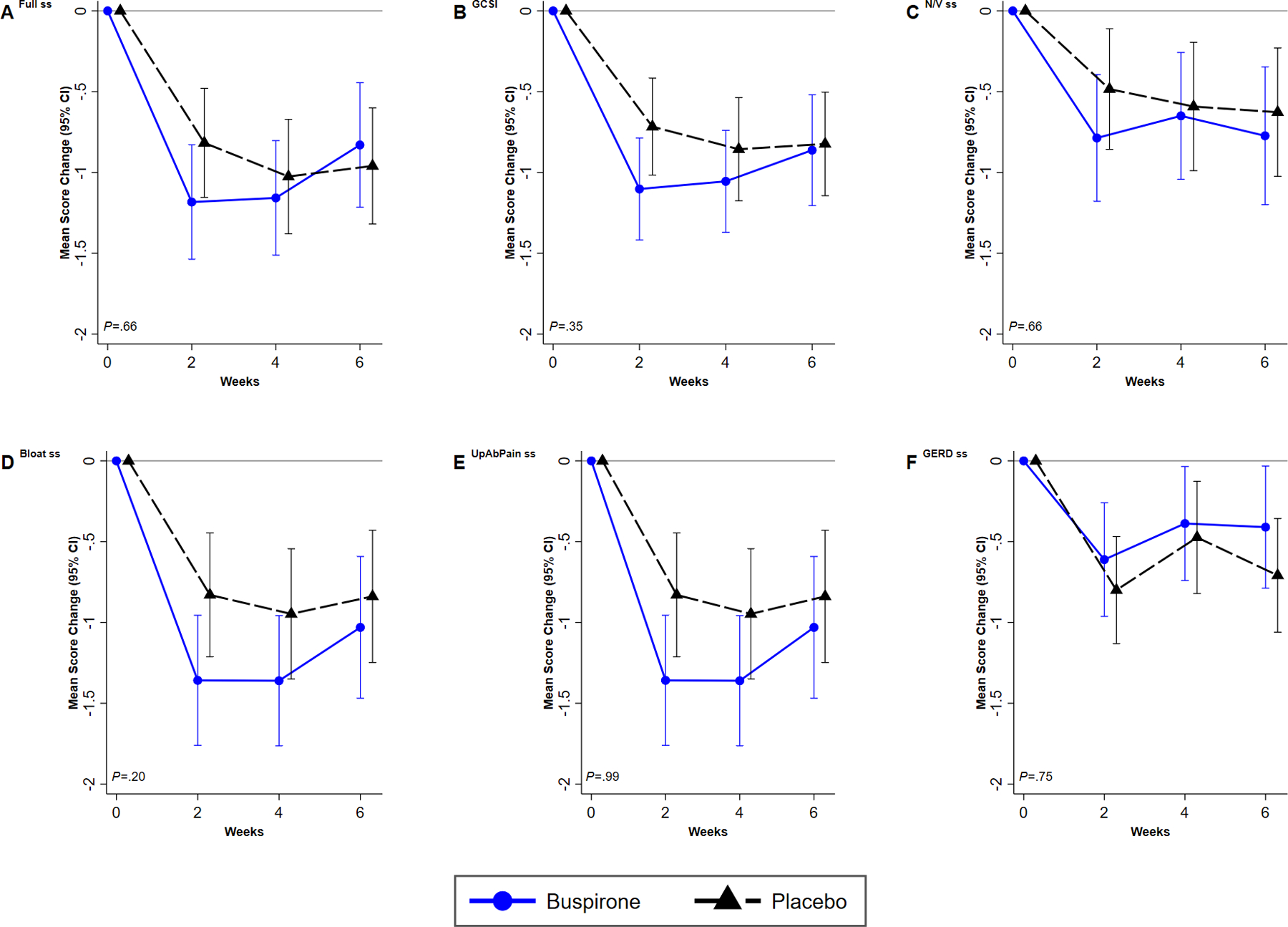
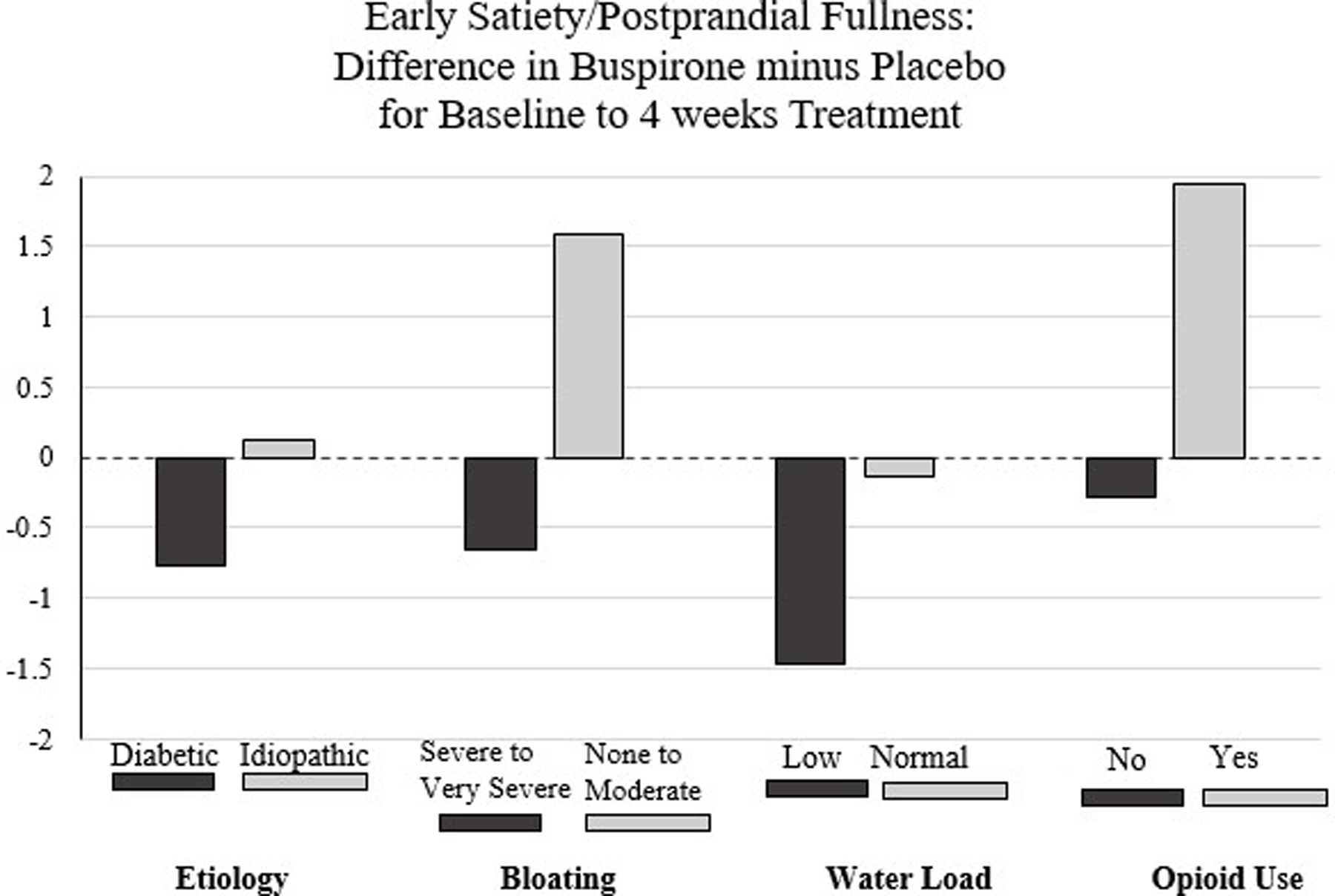
Results and conclusions: Ninety-six patients (47 buspirone, 49 placeboes; 92% female, 50% delayed gastric emptying, 39% diabetic) were enrolled. There was no between-groups difference in the 4-week ES/PPF primary outcome: -1.16 ± 1.25 (SD) on buspirone vs -1.03 ± 1.29 (SD) on placebo (mean DoD: -0.11 [95% CI: -0.68, 0.45]; p = 0.69). Buspirone performed better than placebo in patients with severe-to-very severe bloating at baseline compared to patients with none to moderate: (ES/PPF DoD = -0.65 vs. 1.58, pTX*GROUP = 0.003; pBF = 0.07). Among individual GCSI symptoms, only bloating appeared to improve with buspirone vs. placebo.
Conclusions: Patients with moderate-to-severe early satiety/postprandial fullness and other symptoms of gastroparesis did not benefit from buspirone treatment to improve the ES/PPF primary outcome compared with placebo. There was a suggestion of the benefit of buspirone in patients with more severe bloating.
Trial registration: ClinicalTrials.gov NCT0358714285.
© 2023 John Wiley & Sons Ltd.
Conflict of interest statement
Competing Interests: the authors have no competing interests.
Figures
Comment in
-
Editorial: buspirone for gastroparesis-an intriguing option for a challenging condition.Aliment Pharmacol Ther. 2023 Jun;57(11):1347-1348. doi: 10.1111/apt.17511. Aliment Pharmacol Ther. 2023. PMID: 37161626 No abstract available.
-
Letter: interpretation of the BESST trial in the context of baseline antidepressant and neuromodulator use.Aliment Pharmacol Ther. 2024 Jan;59(2):291-292. doi: 10.1111/apt.17800. Aliment Pharmacol Ther. 2024. PMID: 38153276 Free PMC article. No abstract available.
References
-
- Parkman HP, Hasler WL, Fisher RS. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004;127:1592–1622. - PubMed
-
- Parkman HP, Hallinan EK, Hasler WL, et al.; NIDDK Gastroparesis Clinical Research Consortium (GpCRC). Early satiety and postprandial fullness in gastroparesis correlate with gastroparesis severity, gastric emptying, and water load testing. Neurogastroenterol Motil 2017. Apr;29(4). doi: 10.1111/nmo.12981. - DOI - PMC - PubMed
-
- Stanghellini V, Tack J. Gastroparesis: separate entity or just a part of dyspepsia? Gut 2014;63:1972–8. - PubMed
-
- Pasricha PJ, Colvin R, Yates K, Hasler WL, Abell TL, Ünalp-Arida A, Nguyen L, Farrugia G, Koch KL, Parkman HP, Snape WJ, Lee L, Tonascia J, Hamilton F and The NIDDK Gastroparesis Clinical Research Consortium (GpCRC). Clinical characteristics of patients with chronic unexplained nausea and vomiting and normal gastric emptying. Clin Gastroenterol Hepatol 2011;9:567–576 - PMC - PubMed
-
- Kelly KA. Gastric emptying of liquids and solids: roles of proximal and distal stomach. Am J Physiol 1980;239:G71–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous