

Effectiveness of an Over-the-Counter Self-fitting Hearing Aid Compared With an Audiologist-Fitted Hearing Aid: A Randomized Clinical Trial
- PMID: 37052929
- PMCID: PMC10102918
- DOI: 10.1001/jamaoto.2023.0376
Effectiveness of an Over-the-Counter Self-fitting Hearing Aid Compared With an Audiologist-Fitted Hearing Aid: A Randomized Clinical Trial
Abstract
Importance: Hearing loss is a highly prevalent condition, with numerous debilitating consequences when left untreated. However, less than 20% of US adults with hearing loss use hearing aids. Over-the-counter (OTC) hearing aids became available in October 2022 to improve access and affordability. However, clinical effectiveness studies of available OTC hearing aids using the existing devices in the market are limited.
Objective: To compare the clinical effectiveness of a self-fitting OTC hearing aid with remote support and a hearing aid fitted using audiologist-fitted best practices.
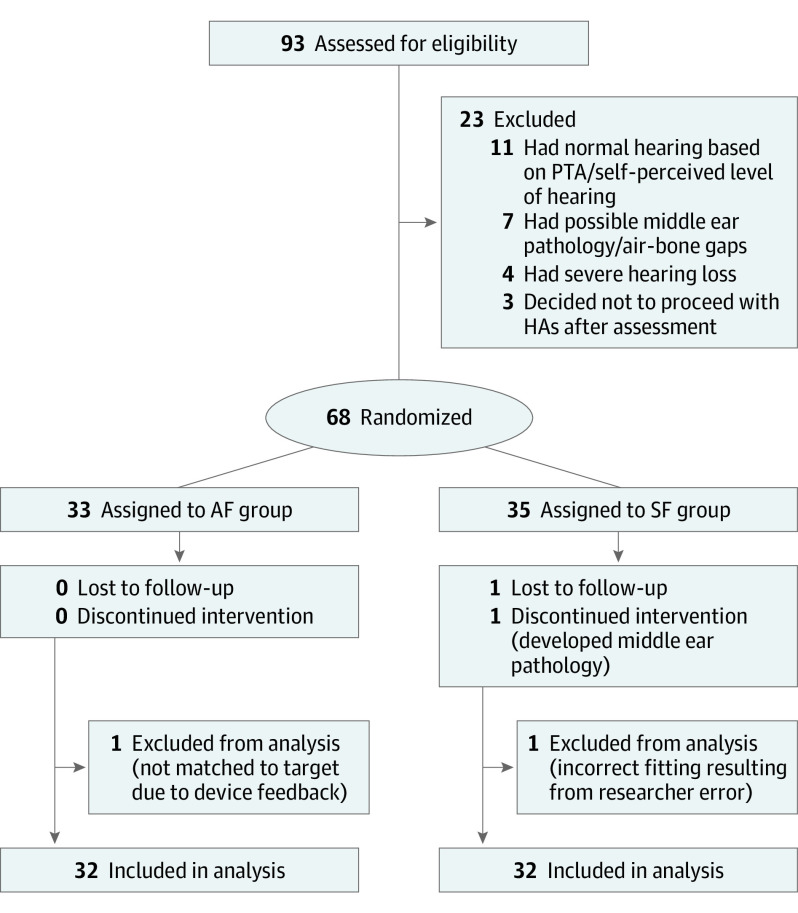
Design, setting, and participants: This randomized clinical effectiveness trial was conducted between April 14 and August 29, 2022. Sixty-eight adults with self-perceived mild to moderate hearing loss were recruited and randomly assigned to either the self-fitting or the audiologist-fitted group. Following bilateral hearing aid fitting, participants first completed a 2-week, take-home field trial without any support. Access to fine-tuning for both groups was only available after the 2-week trial. Support and adjustment were provided remotely for the self-fitting group per request and by the audiologist for the audiologist-fitted group. Participants were then reassessed after an additional 4-week take-home trial.
Interventions: A commercially available self-fitting OTC hearing aid was provided to participants in the self-fitting group who were expected to set up the hearing aids using the commercially supplied instructional material and accompanying smartphone application. In the audiologist-fitted group, audiologists fitted the same hearing aid according to the National Acoustics Laboratories nonlinear version 2 algorithm for prescriptive gain target using real-ear verification with hearing aid use instruction.
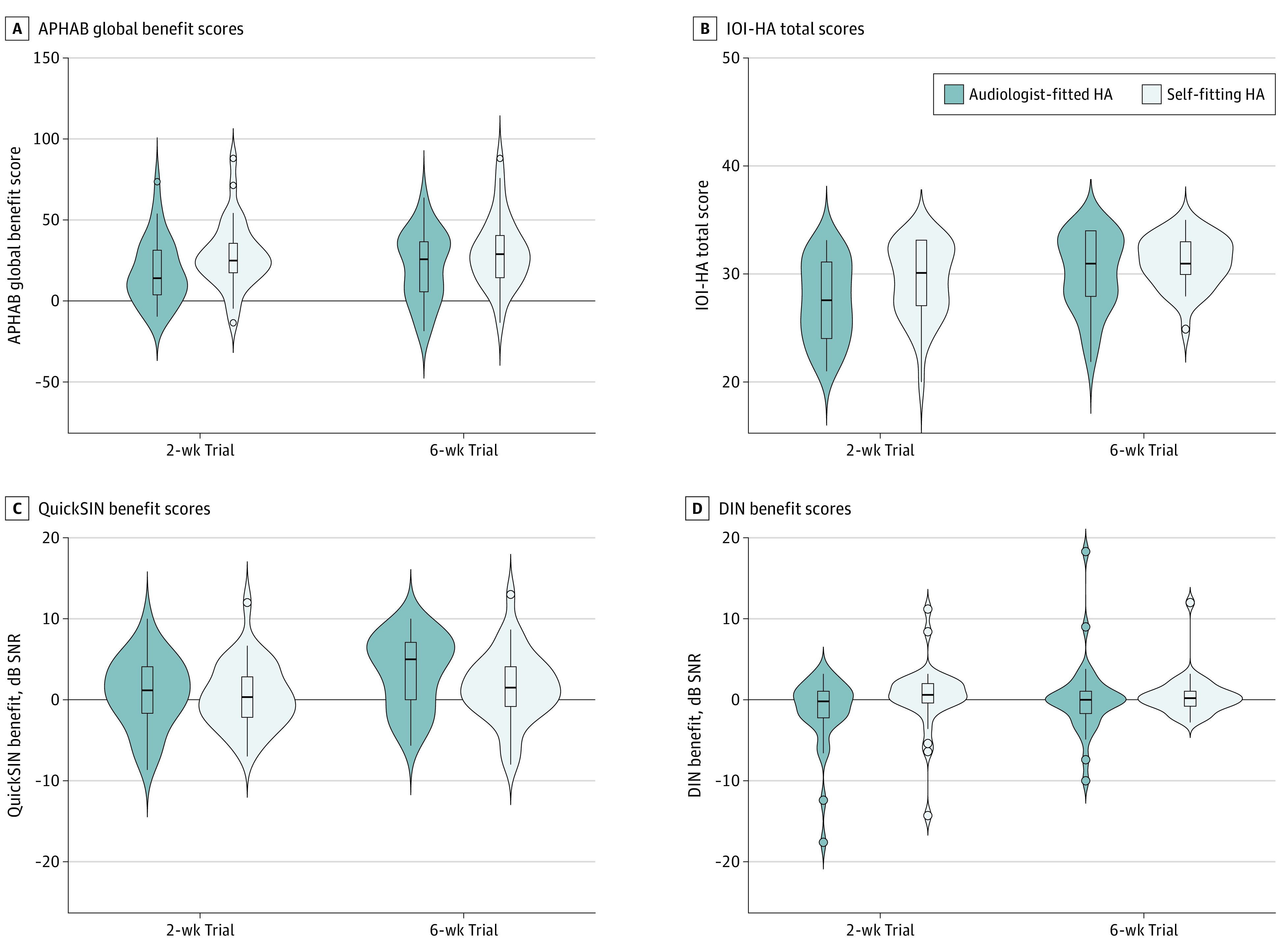
Main outcomes and measures: The primary outcome measure was self-reported hearing aid benefit, measured using the Abbreviated Profile of Hearing Aid Benefit (APHAB). Secondary measures included the International Outcome Inventory for Hearing Aids (IOI-HA) and speech recognition in noise measured using an abbreviated speech-in-noise test and a digits-in-noise test. All measures were completed at baseline and at 2 intervals following hearing aid fitting (2 and 6 weeks).
Results: Sixty-four participants were included in the analytic sample (33 men [51.6%]; mean [SD] age, 63.6 [14.1] years), with equal numbers of participants (n = 32) randomized into each group. The groups did not differ significantly in age (effect size r = -0.2 [95% CI, -0.3 to 0.2]) or 4-frequency pure-tone average (effect size r = 0.2 [95% CI, -0.1 to 0.4]). After the 2-week field trial, the self-fitting group had an initial advantage compared with the audiologist-fitted group on the self-reported APHAB (Cohen d = -0.5 [95% CI, -1.0 to 0]) and IOI-HA (effect size r = 0.3 [95% CI, 0.0-0.5]) but not speech recognition in noise. At the end of the 6-week trial, no meaningful differences were evident between the groups on any outcome measures.
Conclusion and relevance: In this randomized clinical effectiveness trial, self-fitting OTC hearing aids with remote support yielded outcomes at 6 weeks post fitting comparable to those of hearing aids fitted using audiologist best practices. These findings suggest that self-fitting OTC hearing aids may provide an effective intervention for mild to moderate hearing loss.
Trial registration: ClinicalTrials.gov Identifier: NCT05337748.
Conflict of interest statement
Figures
References
-
- World Health Organization. World report on hearing. March 3, 2021. Accessed July 7, 2021. https://www.who.int/publications/i/item/9789240020481
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
