

Short-term topiramate treatment prevents radiation-induced cytotoxic edema in preclinical models of breast-cancer brain metastasis
- PMID: 37053041
- PMCID: PMC10547511
- DOI: 10.1093/neuonc/noad070
Short-term topiramate treatment prevents radiation-induced cytotoxic edema in preclinical models of breast-cancer brain metastasis
Abstract
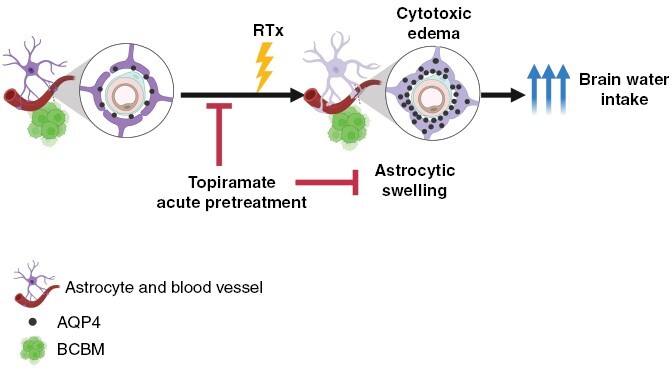
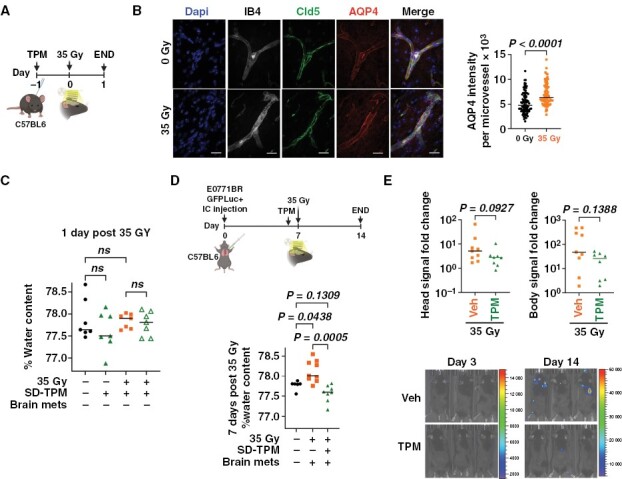
Background: Brain edema is a common complication of brain metastases (BM) and associated treatment. The extent to which cytotoxic edema, the first step in the sequence that leads to ionic edema, vasogenic edema, and brain swelling, contributes to radiation-induced brain edema during BM remains unknown. This study aimed to determine whether radiation-associated treatment of BM induces cytotoxic edema and the consequences of blocking the edema in preclinical models of breast-cancer brain metastases (BCBM).
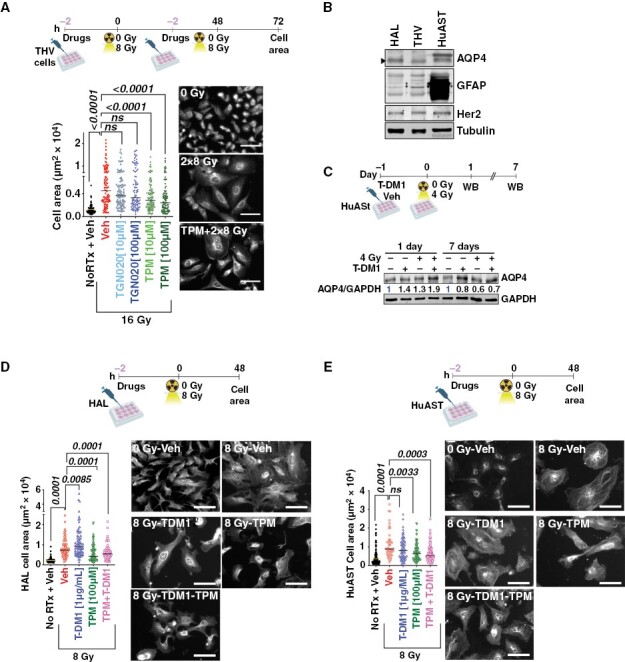
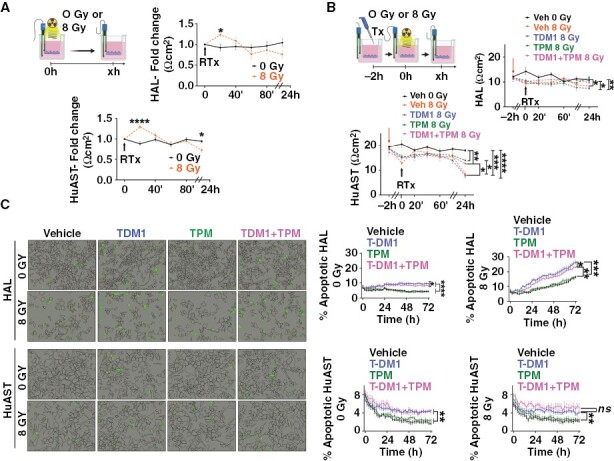
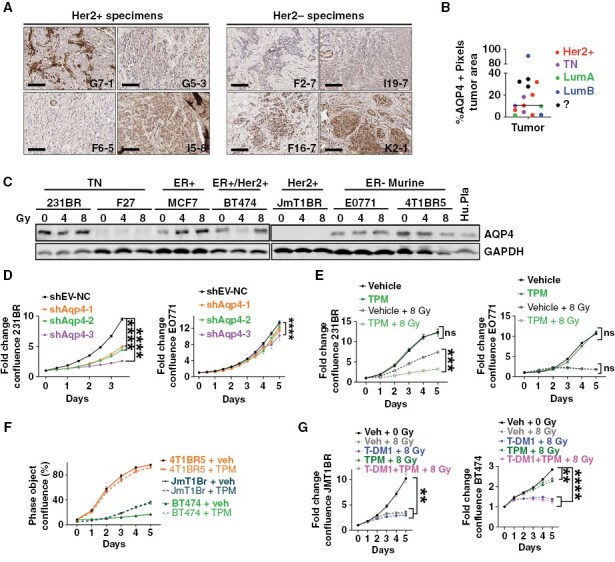
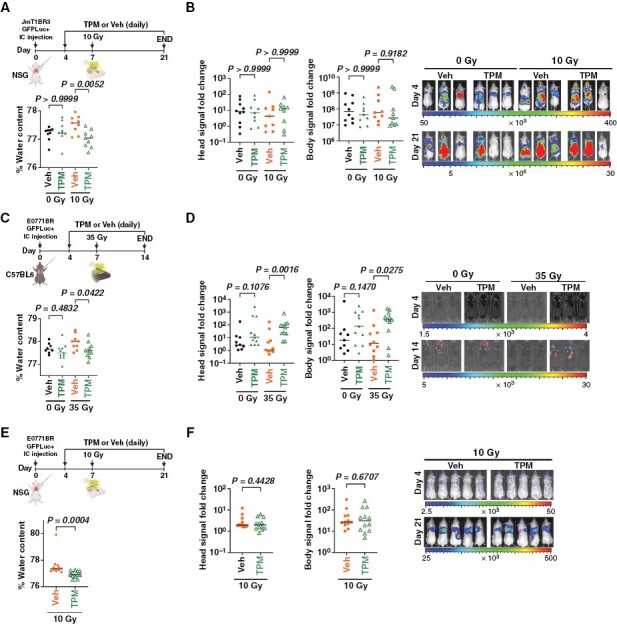
Methods: Using in vitro and in vivo models, we measured astrocytic swelling, trans-electric resistance (TEER), and aquaporin 4 (AQP4) expression following radiation. Genetic and pharmacological inhibition of AQP4 in astrocytes and cancer cells was used to assess the role of AQP4 in astrocytic swelling and brain water intake. An anti-epileptic drug that blocks AQP4 function (topiramate) was used to prevent cytotoxic edema in models of BM.
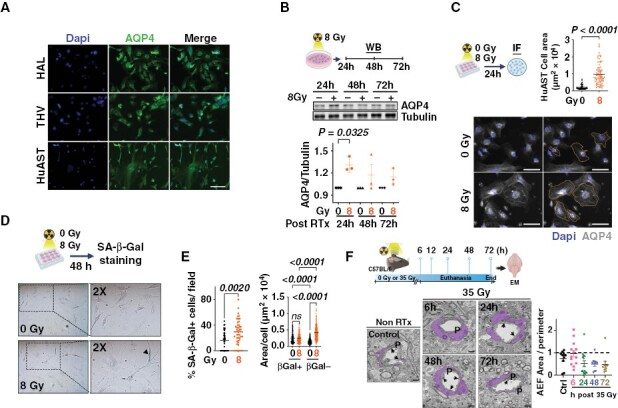
Results: Radiation-induced astrocytic swelling and transient upregulation of AQP4 occurred within the first 24 hours following radiation. Topiramate decreased radiation-induced astrocytic swelling and loss of TEER in astrocytes in vitro, and acute short-term treatment (but not continuous administration), prevented radiation-induced increase in brain water content without pro-tumorigenic effects in multiple preclinical models of BCBM. AQP4 was expressed in clinical BM and breast-cancer cell lines, but AQP4 targeting had limited direct pro-tumorigenic or radioprotective effects in cancer cells that could impact its clinical translation.
Conclusions: Patients with BM could find additional benefits from acute and temporary preventive treatment of radiation-induced cytotoxic edema using anti-epileptic drugs able to block AQP4 function.
Keywords: Aquaporin 4; Brain Edema; Brain metastasis; Brain radiation; Cytotoxic Edema; Topiramate.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
MJC, DMC, KA, JAJ, ZL, and NT: no conflicts. DRO: Clinical trial research funding from Integra Biosciences, Servier Pharmaceuticals. SDK: Clinical trial, preclinical research funding from AstraZeneca, Genentech, Ionis and Roche Pharmaceuticals are all unrelated to this work. PK: Clinical research grant support from Genentech, Radius Health, and Eli Lilly all unrelated to this work.
Figures
Update of
-
Short-term Topiramate treatment prevents radiation-induced cytotoxic edema in preclinical models of breast-cancer brain metastasis.bioRxiv [Preprint]. 2023 Feb 15:2023.02.14.528559. doi: 10.1101/2023.02.14.528559. bioRxiv. 2023. Update in: Neuro Oncol. 2023 Oct 3;25(10):1802-1814. doi: 10.1093/neuonc/noad070. PMID: 36824740 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
