

Endothelial Cell Dysfunction and Increased Cardiovascular Risk in Patients With Chronic Kidney Disease
- PMID: 37053275
- PMCID: PMC10097498
- DOI: 10.1161/CIRCRESAHA.123.321752
Endothelial Cell Dysfunction and Increased Cardiovascular Risk in Patients With Chronic Kidney Disease
Abstract
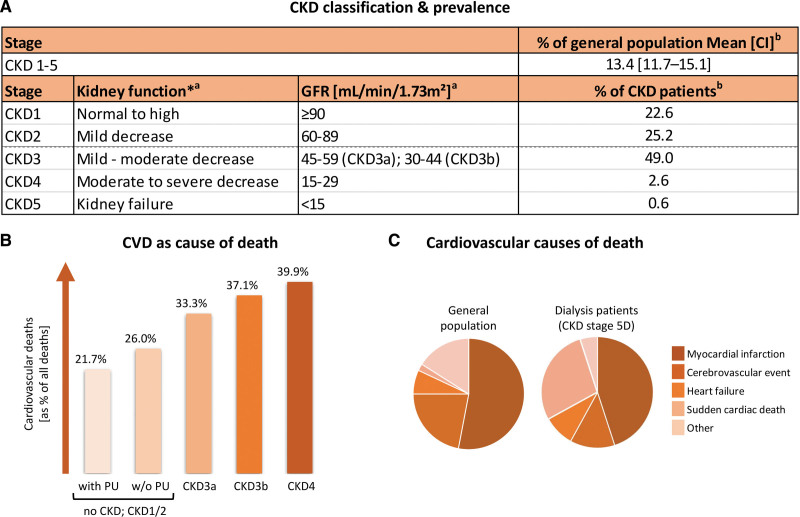
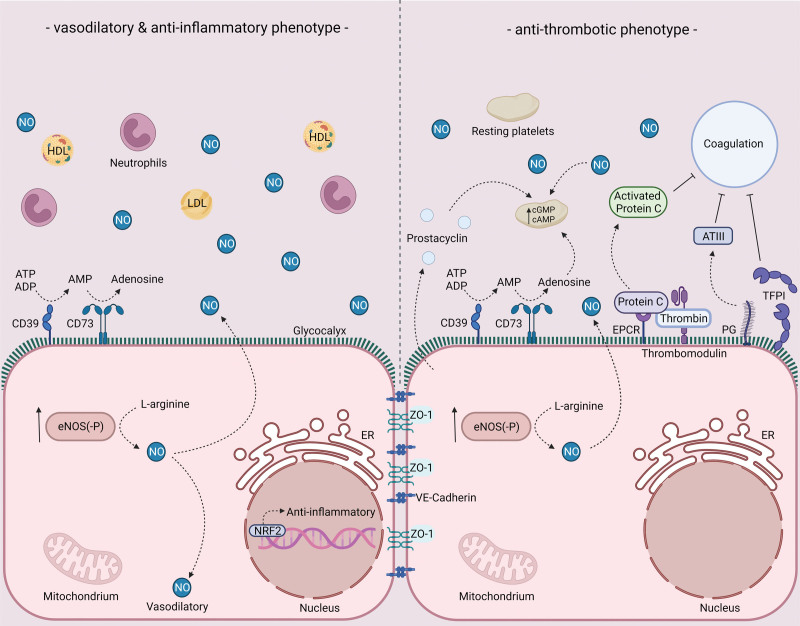
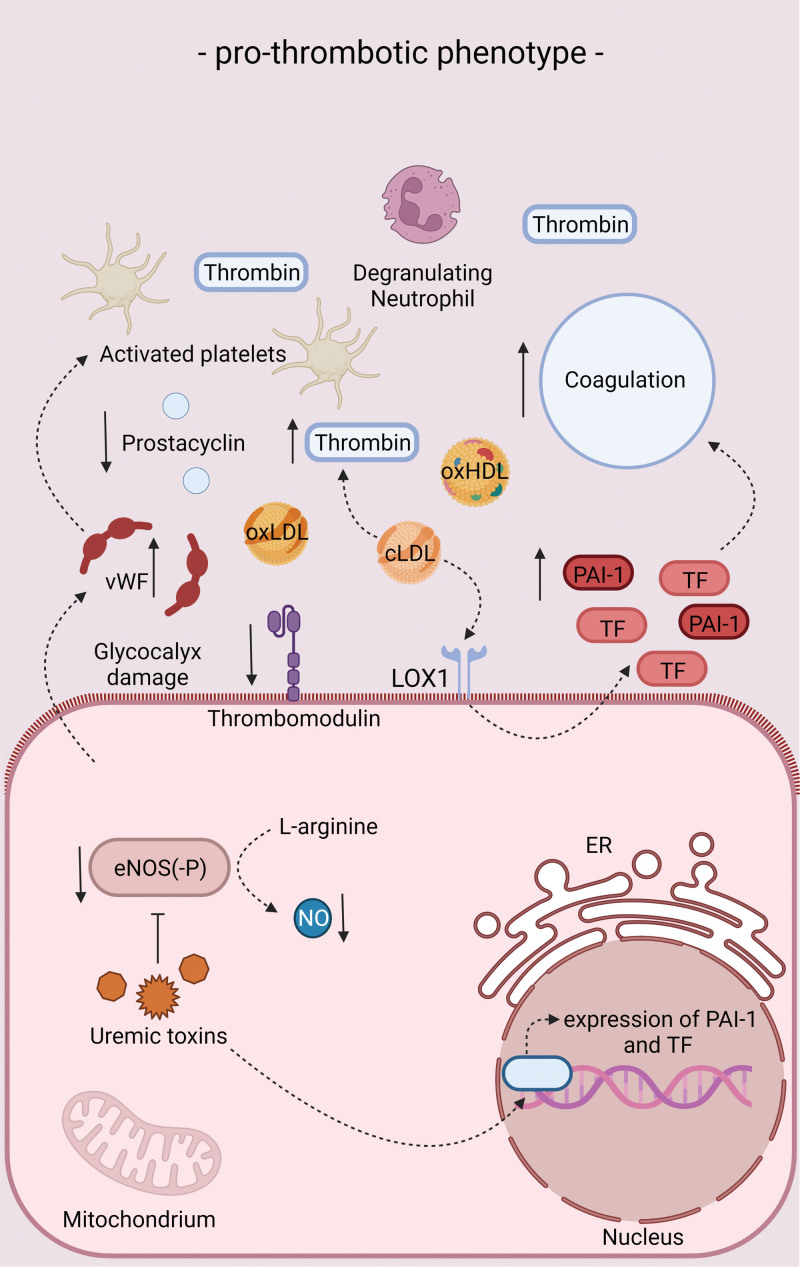
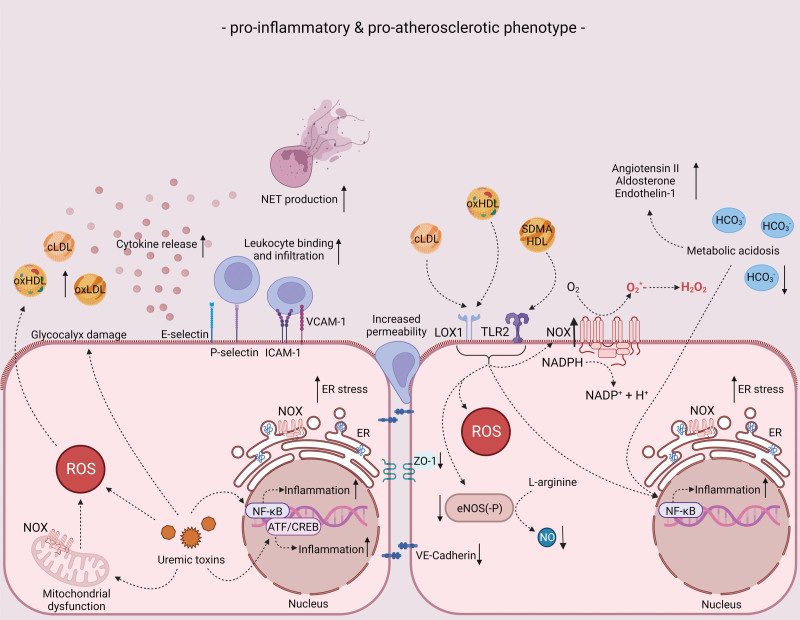
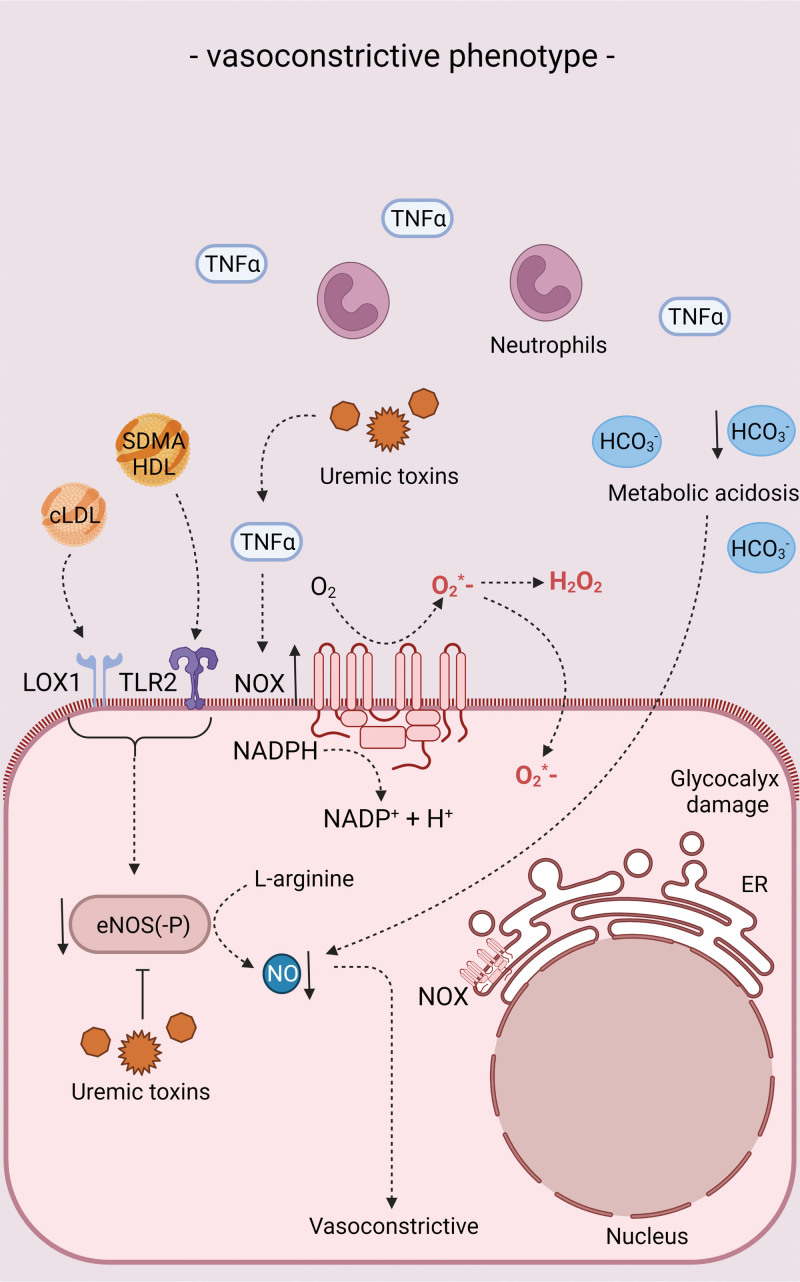
The endothelium is considered to be the gatekeeper of the vessel wall, maintaining and regulating vascular integrity. In patients with chronic kidney disease, protective endothelial cell functions are impaired due to the proinflammatory, prothrombotic and uremic environment caused by the decline in kidney function, adding to the increase in cardiovascular complications in this vulnerable patient population. In this review, we discuss endothelial cell functioning in healthy conditions and the contribution of endothelial cell dysfunction to cardiovascular disease. Further, we summarize the phenotypic changes of the endothelium in chronic kidney disease patients and the relation of endothelial cell dysfunction to cardiovascular risk in chronic kidney disease. We also review the mechanisms that underlie endothelial changes in chronic kidney disease and consider potential pharmacological interventions that can ameliorate endothelial health.
Keywords: atherosclerosis; cardiovascular diseases; chronic kidney diseases; endothelial cells; vascular stiffness.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, Kurella Tamura M, Feldman HI. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63:713–735. doi: 10.1053/j.ajkd.2014.01.416 - PubMed
-
- Roberts MA, Polkinghorne KR, McDonald SP, Ierino FL. Secular trends in cardiovascular mortality rates of patients receiving dialysis compared with the general population. Am J Kidney Dis. 2011;58:64–72. doi: 10.1053/j.ajkd.2011.01.024 - PubMed
-
- van der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey A, de Jong P, Gansevoort RT, Matsushita K, Coresh J, et al. ; Chronic Kidney Disease Prognosis Consortium. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79:1341–1352. doi: 10.1038/ki.2010.536 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
