

Dual-Layer Detector Cone-Beam CT Angiography for Stroke Assessment: First-in-Human Results (the Next Generation X-ray Imaging System Trial)
- PMID: 37055159
- PMCID: PMC10171384
- DOI: 10.3174/ajnr.A7835
Dual-Layer Detector Cone-Beam CT Angiography for Stroke Assessment: First-in-Human Results (the Next Generation X-ray Imaging System Trial)
Erratum in
-
Erratum.AJNR Am J Neuroradiol. 2023 Jul;44(7):E32. doi: 10.3174/ajnr.A7898. Epub 2023 May 25. AJNR Am J Neuroradiol. 2023. PMID: 37230541 Free PMC article. No abstract available.
Abstract
Background and purpose: In patients with stroke, IV cone-beam CTA in the angiography suite could be an alternative to CTA to shorten the door-to-thrombectomy time. However, image quality in cone-beam CTA is typically limited by artifacts. This study evaluated a prototype dual-layer detector cone-beam CT angiography versus CTA in patients with stroke.
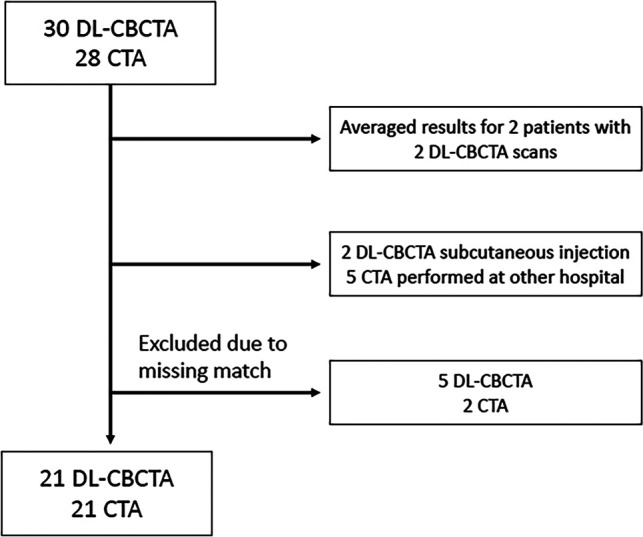
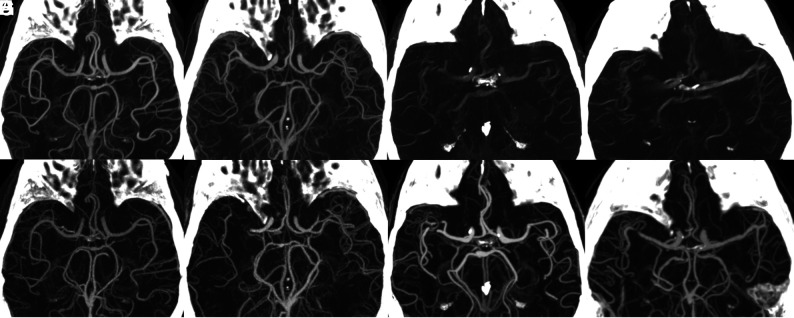
Materials and methods: A prospective, single-center trial enrolled consecutive patients with ischemic or hemorrhagic stroke on initial CT. Intracranial arterial segment vessel conspicuity and artifact presence were evaluated on dual-layer cone-beam CTA 70-keV virtual monoenergetic images and CTA. Eleven predetermined vessel segments were matched for every patient. Twelve patients were necessary to show noninferiority to CTA. Noninferiority was determined by the exact binomial test; the 1-sided lower performance boundary was prospectively set to 80% (98.75% CI).
Results: Twenty-one patients had matched image sets (mean age, 72 years). After excluding examinations with movement or contrast media injection issues, all readers individually considered dual-layer cone-beam CT angiography noninferior to CTA (CI boundary, 93%, 84%, 80%, respectively) when evaluating arteries relevant in candidates for intracranial thrombectomy. Artifacts were more prevalent compared with CTA. The majority assessment rated each individual segment except M1 as having noninferior conspicuity compared with CTA.
Conclusions: In a single-center stroke setting, dual-layer detector cone-beam CTA virtual monoenergetic images are noninferior to CTA under certain conditions. Notably, the prototype is hampered by a long scan time and is not capable of contrast media bolus tracking. After excluding examinations with such scan issues, readers considered dual-layer detector cone-beam CTA noninferior to CTA, despite more artifacts.
© 2023 by American Journal of Neuroradiology.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical