

Leflunomide treatment for patients hospitalised with COVID-19: DEFEAT-COVID randomised controlled trial
- PMID: 37055207
- PMCID: PMC10105917
- DOI: 10.1136/bmjopen-2022-068179
Leflunomide treatment for patients hospitalised with COVID-19: DEFEAT-COVID randomised controlled trial
Abstract
Objective: To evaluate the clinical efficacy and safety of leflunomide (L) added to the standard-of-care (SOC) treatment in COVID-19 patients hospitalised with moderate/critical clinical symptoms.
Design: Prospective, open-label, multicentre, stratified, randomised clinical trial.
Setting: Five hospitals in UK and India, from September 2020 to May 2021.
Participants: Adults with PCR confirmed COVID-19 infection with moderate/critical symptoms within 15 days of onset.
Intervention: Leflunomide 100 mg/day (3 days) followed by 10-20 mg/day (7 days) added to standard care.
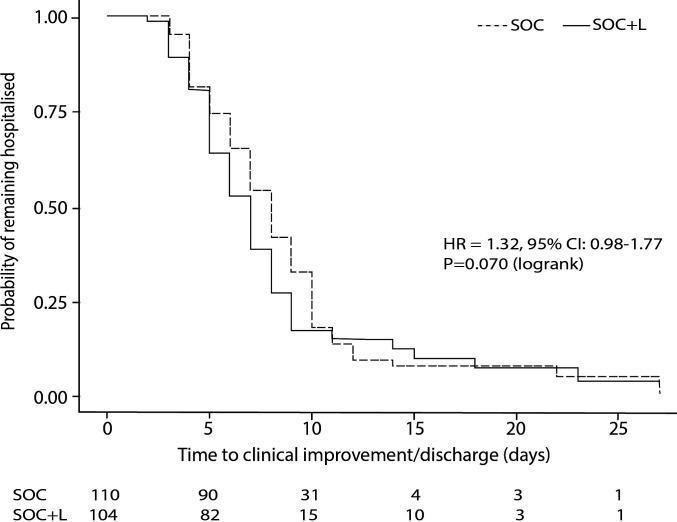
Primary outcomes: The time to clinical improvement (TTCI) defined as two-point reduction on a clinical status scale or live discharge prior to 28 days; safety profile measured by the incidence of adverse events (AEs) within 28 days.
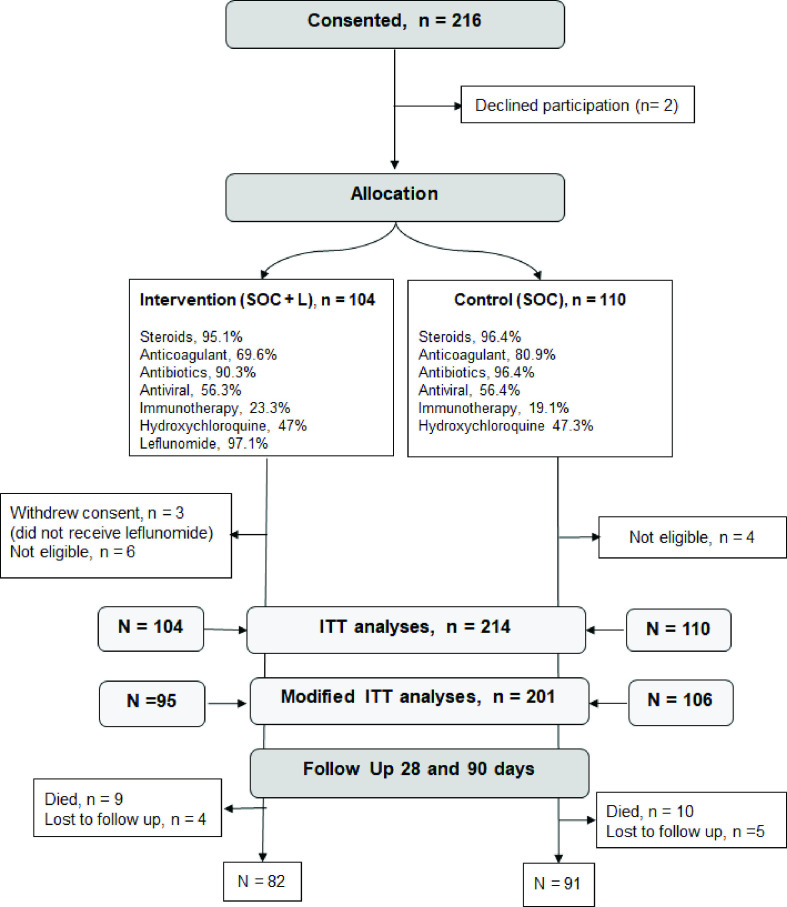
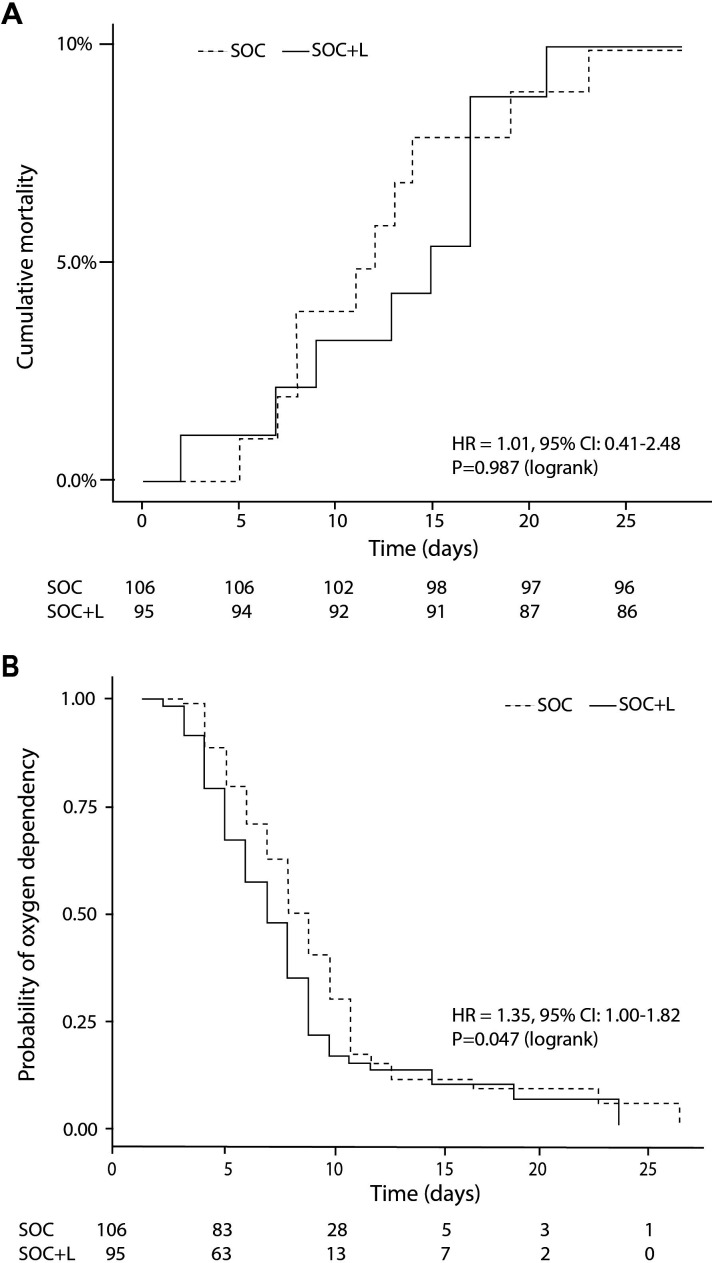
Results: Eligible patients (n=214; age 56.3±14.9 years; 33% female) were randomised to SOC+L (n=104) and SOC group (n=110), stratified according to their clinical risk profile. TTCI was 7 vs 8 days in SOC+L vs SOC group (HR 1.317; 95% CI 0.980 to 1.768; p=0.070). Incidence of serious AEs was similar between the groups and none was attributed to leflunomide. In sensitivity analyses, excluding 10 patients not fulfilling the inclusion criteria and 3 who withdrew consent before leflunomide treatment, TTCI was 7 vs 8 days (HR 1.416, 95% CI 1.041 to 1.935; p=0.028), indicating a trend in favour of the intervention group. All-cause mortality rate was similar between groups, 9/104 vs 10/110. Duration of oxygen dependence was shorter in the SOC+L group being a median 6 days (IQR 4-8) compared with 7 days (IQR 5-10) in SOC group (p=0.047).
Conclusion: Leflunomide, added to the SOC treatment for COVID-19, was safe and well tolerated but had no major impact on clinical outcomes. It may shorten the time of oxygen dependence by 1 day and thereby improve TTCI/hospital discharge in moderately affected COVID-19 patients.
Trial registration numbers: EudraCT Number: 2020-002952-18, NCT05007678.
Keywords: COVID-19; INFECTIOUS DISEASES; Respiratory infections.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO . Available: https://COVID19.who.int/
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical