

A new polygenic score for refractive error improves detection of children at risk of high myopia but not the prediction of those at risk of myopic macular degeneration
- PMID: 37055258
- PMCID: PMC10203044
- DOI: 10.1016/j.ebiom.2023.104551
A new polygenic score for refractive error improves detection of children at risk of high myopia but not the prediction of those at risk of myopic macular degeneration
Abstract
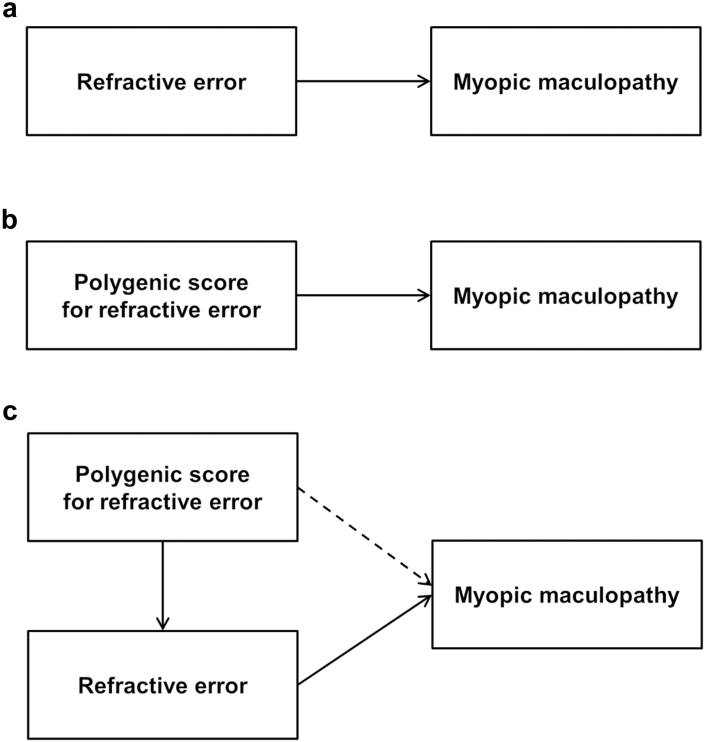
Background: High myopia (HM), defined as a spherical equivalent refractive error (SER) ≤ -6.00 diopters (D), is a leading cause of sight impairment, through myopic macular degeneration (MMD). We aimed to derive an improved polygenic score (PGS) for predicting children at risk of HM and to test if a PGS is predictive of MMD after accounting for SER.
Methods: The PGS was derived from genome-wide association studies in participants of UK Biobank, CREAM Consortium, and Genetic Epidemiology Research on Adult Health and Aging. MMD severity was quantified by a deep learning algorithm. Prediction of HM was quantified as the area under the receiver operating curve (AUROC). Prediction of severe MMD was assessed by logistic regression.
Findings: In independent samples of European, African, South Asian and East Asian ancestry, the PGS explained 19% (95% confidence interval 17-21%), 2% (1-3%), 8% (7-10%) and 6% (3-9%) of the variation in SER, respectively. The AUROC for HM in these samples was 0.78 (0.75-0.81), 0.58 (0.53-0.64), 0.71 (0.69-0.74) and 0.67 (0.62-0.72), respectively. The PGS was not associated with the risk of MMD after accounting for SER: OR = 1.07 (0.92-1.24).
Interpretation: Performance of the PGS approached the level required for clinical utility in Europeans but not in other ancestries. A PGS for refractive error was not predictive of MMD risk once SER was accounted for.
Funding: Supported by the Welsh Government and Fight for Sight (24WG201).
Keywords: ALSPAC; Generation R; Myopia; Polygenic score; UK Biobank.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no potential conflicts of interests relevant to this manuscript. Outside this manuscript, KOM reports consultancy service for Santen and CooperVision; JAG reports membership of the Data Safety Monitoring Board for ‘CHAMPS-UK’ trial of atropine eyedrops for myopia (unpaid) and editorial board service for IOVS, TVST and OPO (unpaid).
Figures




References
-
- Morgan I.G., Ohno-Matsui K., Saw S.M. Myopia. Lancet. 2012;379(9827):1739–1748. - PubMed
-
- Baird P.N., Saw S.M., Lanca C., et al. Myopia. Nat Rev Dis Primers. 2020;6(1):99. - PubMed
-
- Lee S.H., Jung S.J., Ohn Y.H., Chang J.H. Association between refractive errors and horizontal strabismus: the Korea National Health and Nutrition Examination Survey. J AAPOS. 2021;25(6):340.e1–340.e7. - PubMed
-
- Margines J.B., Huang C., Young A., et al. Refractive errors and amblyopia among children screened by the UCLA preschool vision program in Los Angeles county. Am J Ophthalmol. 2020;210:78–85. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
