

Mixed infection of three nontuberculous mycobacteria species identified by metagenomic next-generation sequencing in a patient with peritoneal dialysis-associated peritonitis: a rare case report and literature review
- PMID: 37055720
- PMCID: PMC10099677
- DOI: 10.1186/s12882-023-03156-8
Mixed infection of three nontuberculous mycobacteria species identified by metagenomic next-generation sequencing in a patient with peritoneal dialysis-associated peritonitis: a rare case report and literature review
Abstract
Background: Peritonitis caused by nontuberculous mycobacteria (NTM) is an infrequent but important complication in patients undergoing peritoneal dialysis (PD). There has been no report of mixed infections with multiple NTM. Peritoneal dialysis-associated peritonitis (PDAP) caused by Mycobacterium abscessus is more common than that caused by M. smegmatis and M. goodii.
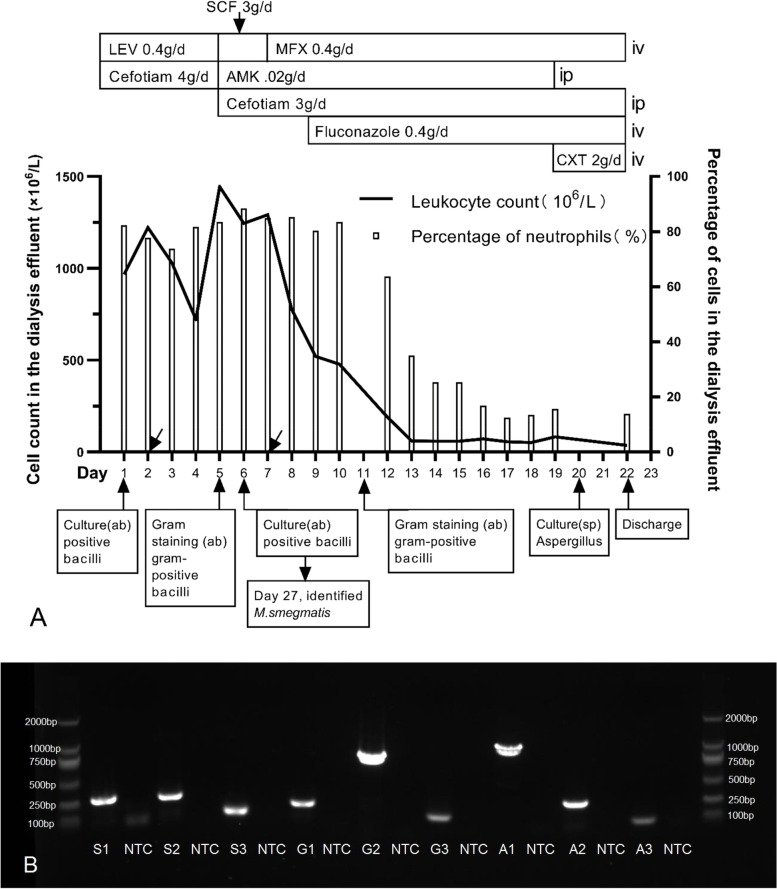
Case presentation: This case concerns a patient with PDAP caused by gram-positive bacilli, which could not be identified at the species level in successive detections of initial peritoneal effluent. Later, M. smegmatis was detected with no sensitivity results in bacterial culture. However, metagenomic next-generation sequencing (mNGS) and first whole-genome sequences indicated that there were three species coexisting in the culture, including M. smegmatis (24,708 reads), M. abscessus (9224 reads), and M. goodii (8305 reads). This is the first case of PDAP with specific evidence that conventional detection methods isolated a poorly pathogenic NTM, whereas mNGS and first whole-genome sequences identified multiple NTM. Pathogenic bacteria might not be detected using conventional methods due to their lower abundance. This case report is the first description of mixed infections with more than two species of NTM during PDAP.
Conclusions: PDAP caused by multiple NTM is rare, and the diagnosis is difficult. When NTM are isolated by conventional tests in patients who are suspected of infection, clinicians should be vigilant, and further tests should be performed to determine the presence of rare or even previously unknown bacteria, for which the quantity is relatively low, but the pathogenicity is high. The rare pathogen may be a primary agent in causing such complications.
Keywords: Case report; Mixed infections; Nontuberculous mycobacteria; Peritoneal dialysis; Peritonitis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Systematic literature review of the diagnosis, prognosis, and treatment of peritoneal dialysis-related infection caused by nontuberculous mycobacteria.BMC Nephrol. 2024 Nov 28;25(1):432. doi: 10.1186/s12882-024-03841-2. BMC Nephrol. 2024. PMID: 39609738 Free PMC article.
-
Peritoneal dialysis-associated infection caused by Mycobacterium abscessus: a case report.BMC Nephrol. 2018 Nov 29;19(1):341. doi: 10.1186/s12882-018-1148-2. BMC Nephrol. 2018. PMID: 30497395 Free PMC article.
-
Mycobacterium abscessus - an uncommon, but important cause of peritoneal dialysis-associated peritonitis - case report and literature review.BMC Nephrol. 2020 Nov 17;21(1):491. doi: 10.1186/s12882-020-02146-4. BMC Nephrol. 2020. PMID: 33203375 Free PMC article. Review.
-
The Clinical Utility of the Neutrophil-to-Lymphocyte Ratio as a Discriminatory Test among Bacterial, Mycobacterium Tuberculosis, and Nontuberculous Mycobacterium Peritoneal Dialysis-Related Peritonitis.Kidney360. 2022 Mar 29;3(6):1031-1038. doi: 10.34067/KID.0000842022. eCollection 2022 Jun 30. Kidney360. 2022. PMID: 35845333 Free PMC article.
-
Nontuberculous mycobacteria infections of peritoneal dialysis patients: A multicenter study.Perit Dial Int. 2021 May;41(3):284-291. doi: 10.1177/0896860820923461. Epub 2020 May 13. Perit Dial Int. 2021. PMID: 32400280
Cited by
-
A Case of Rapidly Diagnosed Mycobacterium intracellulare in a Frail Geriatric Patient With Multimorbidity.Cureus. 2024 Jun 13;16(6):e62313. doi: 10.7759/cureus.62313. eCollection 2024 Jun. Cureus. 2024. PMID: 39006676 Free PMC article.
-
Prevalence of nontuberculous mycobacteria and the emergence of rare species in Henan Province, China.Epidemiol Infect. 2024 May 6;152:e92. doi: 10.1017/S095026882400061X. Epidemiol Infect. 2024. PMID: 38708766 Free PMC article.
-
Culture-Negative Peritonitis and the Latest Diagnostic Techniques.Kidney Dis (Basel). 2024 Dec 2;11(1):25-37. doi: 10.1159/000542870. eCollection 2025 Jan-Dec. Kidney Dis (Basel). 2024. PMID: 40606677 Free PMC article. Review.
-
Clinical efficacy of metagenomic next-generation sequencing for the detection of pathogens in peritoneal dialysis-related peritonitis: a prospective cohort study.Eur J Med Res. 2025 Mar 22;30(1):198. doi: 10.1186/s40001-025-02322-y. Eur J Med Res. 2025. PMID: 40121477 Free PMC article.
-
Targeted deep sequencing of mycobacteria species from extrapulmonary sites not identified by routine line probe assays: A retrospective laboratory analysis of stored clinical cultures.IJID Reg. 2024 Sep 24;13:100464. doi: 10.1016/j.ijregi.2024.100464. eCollection 2024 Dec. IJID Reg. 2024. PMID: 39483154 Free PMC article.
References
-
- Szeto CC, Leung CB, Chow KM, Kwan BC, Law MC, Wang AY, Lui SF, Li PK. Change in bacterial aetiology of peritoneal dialysis-related peritonitis over 10 years: experience from a Centre in South-East Asia. Clin Microbiol Infect. 2005;11(10):837–839. doi: 10.1111/j.1469-0691.2005.01222.x. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
