

A bedside swallowing screen for the identification of post-extubation dysphagia on the intensive care unit - validation of the Gugging Swallowing Screen (GUSS)-ICU
- PMID: 37055724
- PMCID: PMC10099025
- DOI: 10.1186/s12871-023-02072-6
A bedside swallowing screen for the identification of post-extubation dysphagia on the intensive care unit - validation of the Gugging Swallowing Screen (GUSS)-ICU
Abstract
Purpose: Screening for dysphagia at the intensive care unit (ICU) soon after extubation can prevent aspiration, pneumonia, lower mortality, and shorten re-feeding interval. This study aimed to modify the Gugging Swallowing Screen (GUSS), which was developed for acute stroke patients, and to validate it for extubated patients in the ICU.
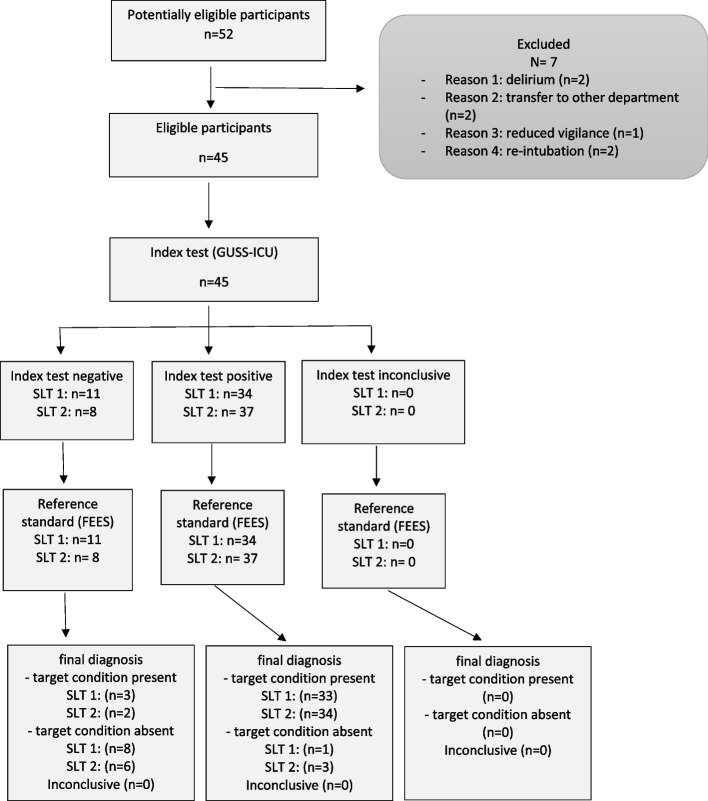
Methods: In this prospective study, forty-five patients who had been intubated for at least 24 h were recruited consecutively at the earliest 24 h after extubation. The modified GUSS-ICU was performed twice by two speech and language therapists independently. Concurrently, gold standard the flexible endoscopic evaluation of swallowing (FEES) was performed by an otorhinolaryngologist. Measurements were conducted within a three-hour period; all testers were blinded to each other's results.
Results: According to FEES, 36 of 45 (80%) participants were diagnosed with dysphagia; 13 of those were severe, 12 moderate, and 11 mild. Compared to FEES, the GUSS-ICU predicted dysphagia well (area under the curve for the initial rater pair: 0.923, 95% CI 0.832-1.000 and 0.923, 95% CI 0.836 -1.000 for the second rater pair). The sensitivity was 91.7% (95% CI 77.5-98.3%) and 94.4% (95% CI 81.3-99.3%); the specificity was 88.9% (51.8-99.7%) and 66.7% (29.9-92.5%); the positive predictive values were 97.1% (83.8-99.5%) and 91.9% (81.7-96.6%), and the negative predictive values were 72.7% (46.8-89%) and 75% (41.9-92.6%) for the first and second rater pairs, respectively. Dysphagia severity classification according to FEES and GUSS-ICU correlated strongly (Spearman's rho: 0.61 for rater 1 and 0.60 for rater 2, p < 0.001). Agreement by all testers was good (Krippendorffs Alpha: 0.73). The interrater reliability showed good agreement (Cohen`s Kappa: 0.84, p < 0.001).
Conclusion: The GUSS-ICU is a simple, reliable, and valid multi-consistency bedside swallowing screen to identify post-extubation dysphagia at the ICU.
Trial registration: ClinicalTrials.gov Identifier: NCT04532398,31/08/2020.
Keywords: Aspiration pneumonia; Gugging Swallowing Screen; Intensive Care Unit; Post-extubation dysphagia; Speech therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
