

Cancer and COVID-19: unravelling the immunological interplay with a review of promising therapies against severe SARS-CoV-2 for cancer patients
- PMID: 37055774
- PMCID: PMC10100631
- DOI: 10.1186/s13045-023-01432-6
Cancer and COVID-19: unravelling the immunological interplay with a review of promising therapies against severe SARS-CoV-2 for cancer patients
Abstract
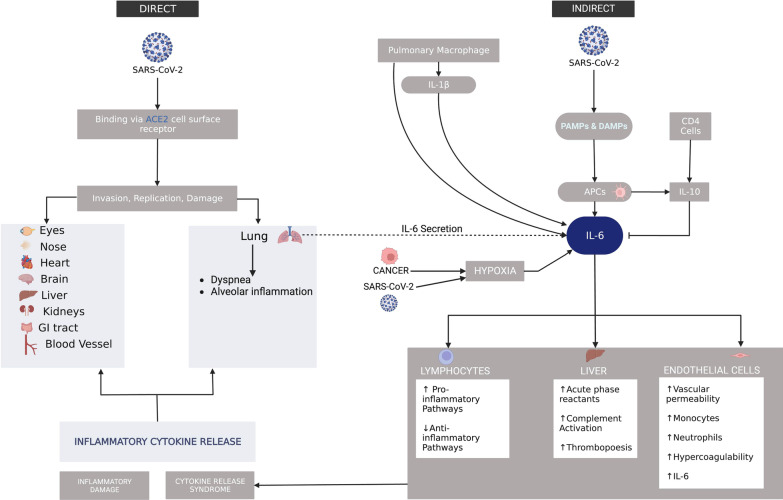
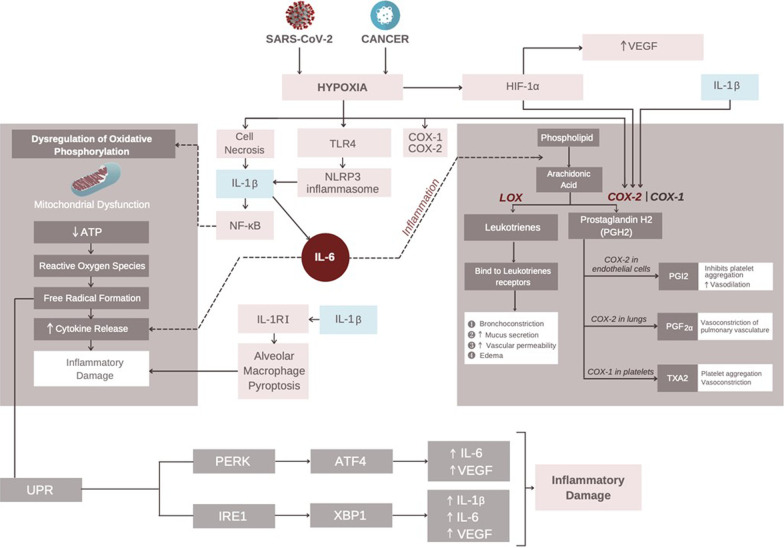
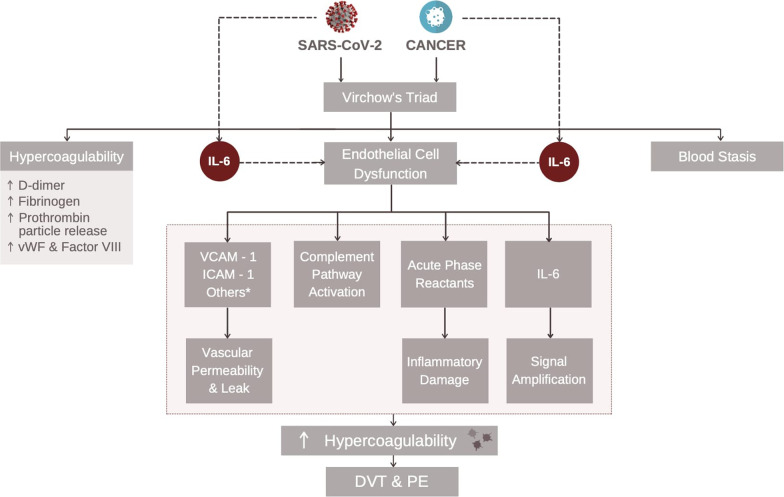
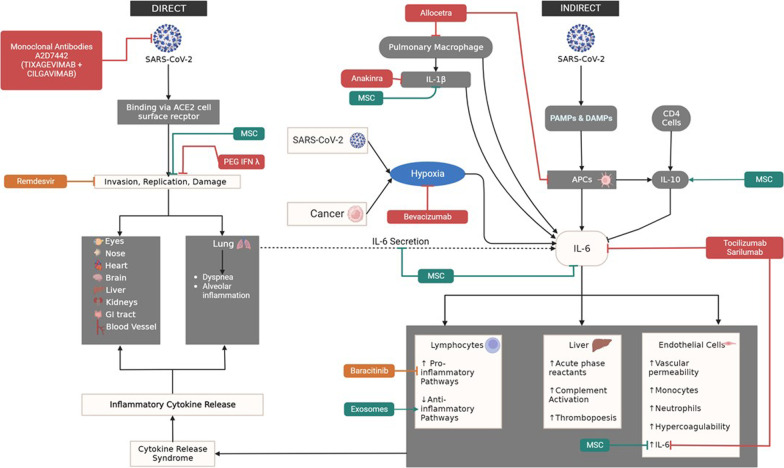
Cancer patients, due to their immunocompromised status, are at an increased risk for severe SARS-CoV-2 infection. Since severe SARS-CoV-2 infection causes multiple organ damage through IL-6-mediated inflammation while stimulating hypoxia, and malignancy promotes hypoxia-induced cellular metabolic alterations leading to cell death, we propose a mechanistic interplay between both conditions that results in an upregulation of IL-6 secretion resulting in enhanced cytokine production and systemic injury. Hypoxia mediated by both conditions results in cell necrosis, dysregulation of oxidative phosphorylation, and mitochondrial dysfunction. This produces free radicals and cytokines that result in systemic inflammatory injury. Hypoxia also catalyzes the breakdown of COX-1 and 2 resulting in bronchoconstriction and pulmonary edema, which further exacerbates tissue hypoxia. Given this disease model, therapeutic options are currently being studied against severe SARS-COV-2. In this study, we review several promising therapies against severe disease supported by clinical trial evidence-including Allocetra, monoclonal antibodies (Tixagevimab-Cilgavimab), peginterferon lambda, Baricitinib, Remdesivir, Sarilumab, Tocilizumab, Anakinra, Bevacizumab, exosomes, and mesenchymal stem cells. Due to the virus's rapid adaptive evolution and diverse symptomatic manifestation, the use of combination therapies offers a promising approach to decrease systemic injury. By investing in such targeted interventions, cases of severe SARS-CoV-2 should decrease along with its associated long-term sequelae and thereby allow cancer patients to resume their treatments.
Keywords: COVID-19; Cancer; Hypoxia; IL-6; SARS-CoV-2; Therapeutics.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Genotypic and predicted phenotypic analysis of SARS-COV-2 Omicron subvariants in immunocompromised patients with COVID-19 following tixagevimab-cilgavimab prophylaxis.J Clin Virol. 2023 Mar;160:105382. doi: 10.1016/j.jcv.2023.105382. Epub 2023 Jan 26. J Clin Virol. 2023. PMID: 36731147 Free PMC article.
-
Treatment of severely ill COVID-19 patients with anti-interleukin drugs (COV-AID): A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Jun 3;21(1):468. doi: 10.1186/s13063-020-04453-5. Trials. 2020. PMID: 32493441 Free PMC article.
-
Interleukin-6 in SARS-CoV-2 induced disease: Interactions and therapeutic applications.Biomed Pharmacother. 2022 Jan;145:112419. doi: 10.1016/j.biopha.2021.112419. Epub 2021 Nov 12. Biomed Pharmacother. 2022. PMID: 34781146 Free PMC article. Review.
-
Coronavirus-19 (SARS-CoV-2) induces acute severe lung inflammation via IL-1 causing cytokine storm in COVID-19: a promising inhibitory strategy.J Biol Regul Homeost Agents. 2020 Nov-Dec;34(6):1971-1975. doi: 10.23812/20-1-E. J Biol Regul Homeost Agents. 2020. PMID: 33016027
-
Pathogenesis-directed therapy of 2019 novel coronavirus disease.J Med Virol. 2021 Mar;93(3):1320-1342. doi: 10.1002/jmv.26610. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33073355 Review.
Cited by
-
COVID-19 Antibody Seroconversion in Cancer Patients: Impact of Therapy Cessation-A Single-Center Study.Vaccines (Basel). 2023 Oct 30;11(11):1659. doi: 10.3390/vaccines11111659. Vaccines (Basel). 2023. PMID: 38005991 Free PMC article.
-
Exosomes derived from syncytia induced by SARS-2-S promote the proliferation and metastasis of hepatocellular carcinoma cells.Front Cell Infect Microbiol. 2025 Jan 8;14:1415356. doi: 10.3389/fcimb.2024.1415356. eCollection 2024. Front Cell Infect Microbiol. 2025. PMID: 39844837 Free PMC article.
-
Tixagevimab/Cilgavimab as Pre-Exposure Prophylaxis against COVID-19 for Multiple Myeloma Patients: A Prospective Study in the Omicron Era.Diseases. 2023 Sep 18;11(3):123. doi: 10.3390/diseases11030123. Diseases. 2023. PMID: 37754319 Free PMC article.
-
Single-Cell Transcriptomics Reveals Pre-existing COVID-19 Vulnerability Factors in Lung Cancer Patients.Mol Cancer Res. 2024 Mar 1;22(3):240-253. doi: 10.1158/1541-7786.MCR-23-0692. Mol Cancer Res. 2024. PMID: 38063850 Free PMC article.
-
Hemophagocytic lymphohistiocytosis: current treatment advances, emerging targeted therapy and underlying mechanisms.J Hematol Oncol. 2024 Nov 7;17(1):106. doi: 10.1186/s13045-024-01621-x. J Hematol Oncol. 2024. PMID: 39511607 Free PMC article. Review.
References
-
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) 2021 [Available from: https://coronavirus.jhu.edu/map.html.
-
- Stawicki SP, Jeanmonod R, Miller AC, Paladino L, Gaieski DF, Yaffee AQ, et al. The 2019–2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: a joint american college of academic international medicine-world academic council of emergency medicine multidisciplinary COVID-19 working group consensus paper. J Glob Infect Dis. 2020;12(2):47. doi: 10.4103/jgid.jgid_86_20. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
