

Immunotherapy of thymic epithelial tumors: molecular understandings and clinical perspectives
- PMID: 37055838
- PMCID: PMC10099901
- DOI: 10.1186/s12943-023-01772-4
Immunotherapy of thymic epithelial tumors: molecular understandings and clinical perspectives
Abstract
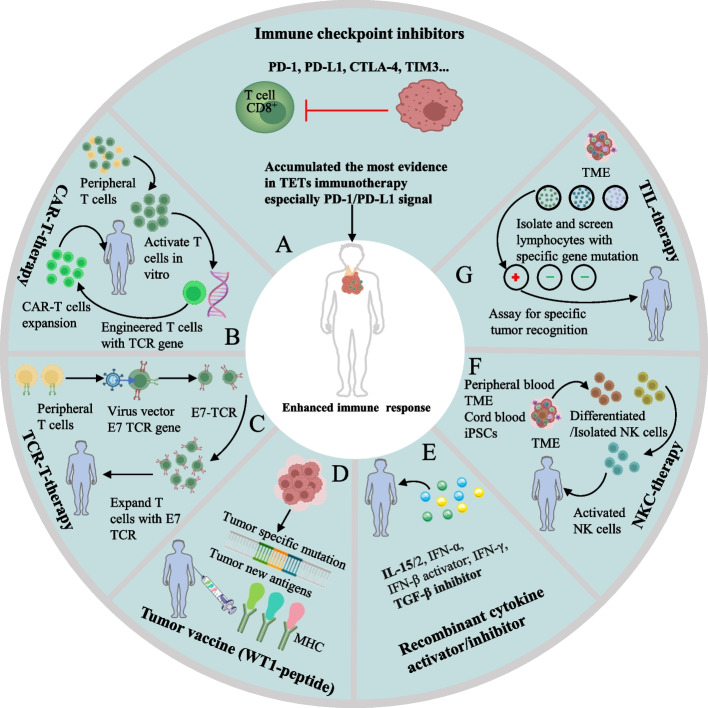
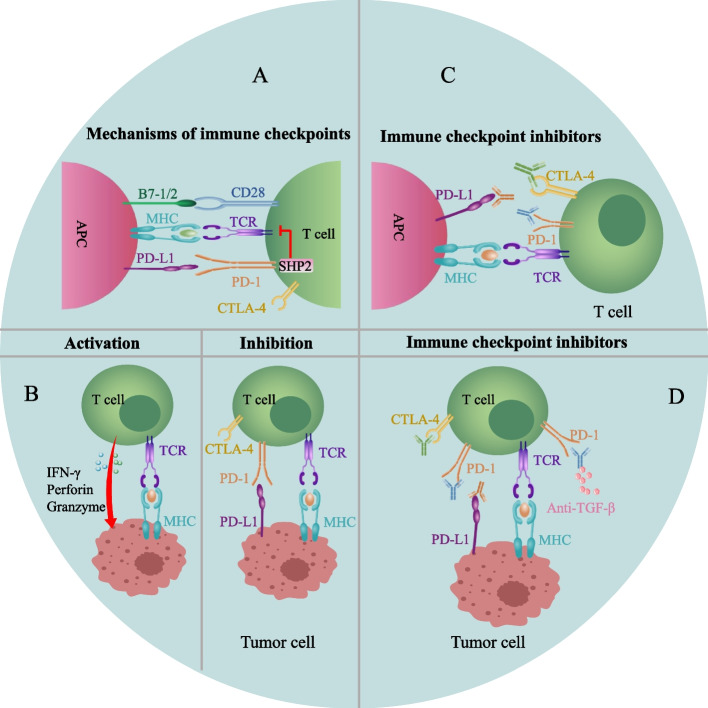
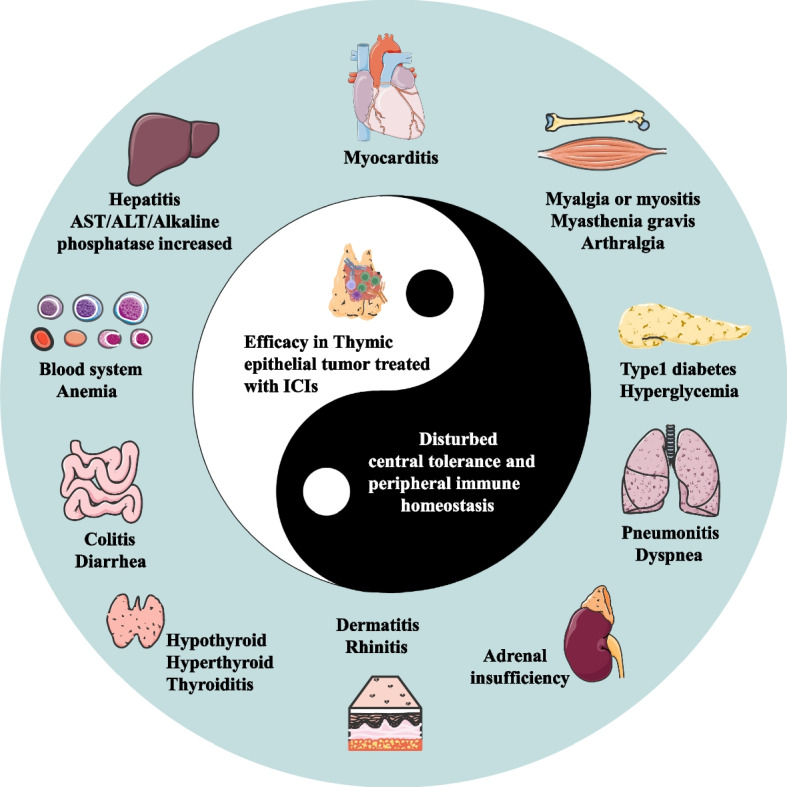
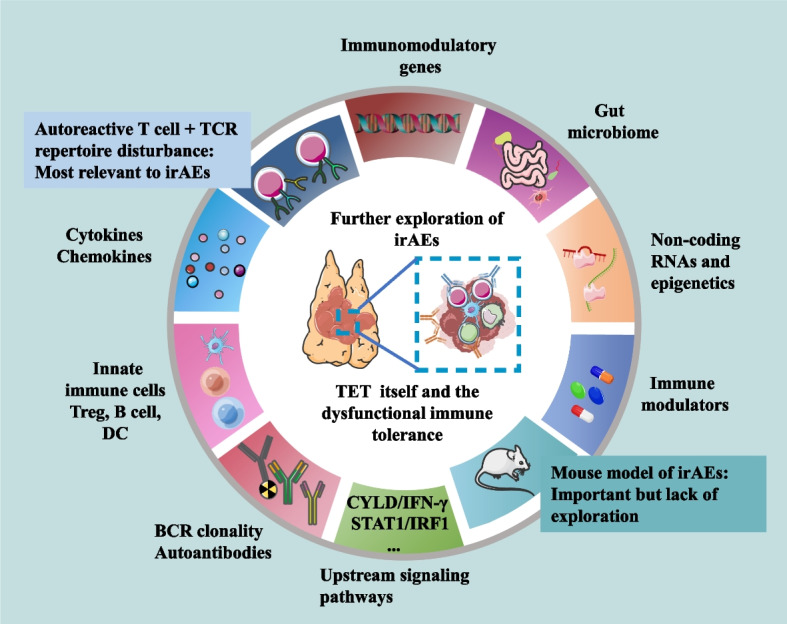
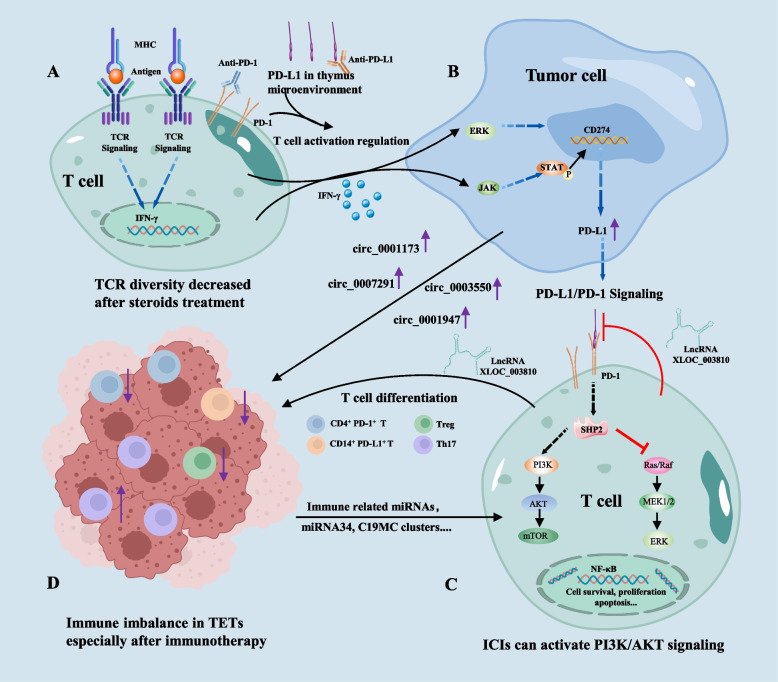
Immunotherapy has emerged to play a rapidly expanding role in the treatment of cancers. Currently, many clinical trials of therapeutic agents are on ongoing with majority of immune checkpoint inhibitors (ICIs) especially programmed death receptor 1 (PD-1) and its ligand 1 (PD-L1) inhibitors. PD-1 and PD-L1, two main immune checkpoints, are expressed at high levels in thymic epithelial tumors (TETs) and could be predictors of the progression and immunotherapeutic efficacy of TETs. However, despite inspiring efficacy reported in clinical trials and clinical practice, significantly higher incidence of immune-related adverse events (irAEs) than other tumors bring challenges to the administration of ICIs in TETs. To develop safe and effective immunotherapeutic patterns in TETs, understanding the clinical properties of patients, the cellular and molecular mechanisms of immunotherapy and irAEs occurrence are crucial. In this review, the progress of both basic and clinical research on immune checkpoints in TETs, the evidence of therapeutic efficacy and irAEs based on PD-1 /PD-L1 inhibitors in TETs treatment are discussed. Additionally, we highlighted the possible mechanisms underlying irAEs, prevention and management strategies, the insufficiency of current research and some worthy research insights. High PD-1/PD-L1 expression in TETs provides a rationale for ICI use. Completed clinical trials have shown an encouraging efficacy of ICIs, despite the high rate of irAEs. A deeper mechanism understanding at molecular level how ICIs function in TETs and why irAEs occur will help maximize the immunotherapeutic efficacy while minimizing irAEs risks in TET treatment to improve patient prognosis.
Keywords: Immune checkpoint inhibitors; Immune-related adverse events; Immunotherapy; PD-1; PD-L1; Thymic epithelial tumors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures

Similar articles
-
The efficacy and safety of immunotherapy in thymic epithelial tumors: more effective, more risky: a systematic review.J Thorac Dis. 2021 Aug;13(8):5093-5103. doi: 10.21037/jtd-21-290. J Thorac Dis. 2021. PMID: 34527346 Free PMC article. Review.
-
Unraveling the complexities of immunotherapy for thymic epithelial tumors via bioinformatics and experimental analyses.Comput Biol Med. 2025 Feb;185:109488. doi: 10.1016/j.compbiomed.2024.109488. Epub 2024 Dec 3. Comput Biol Med. 2025. PMID: 39631109
-
Expression of PD-L1 and other immunotherapeutic targets in thymic epithelial tumors.PLoS One. 2017 Aug 3;12(8):e0182665. doi: 10.1371/journal.pone.0182665. eCollection 2017. PLoS One. 2017. PMID: 28771603 Free PMC article.
-
Understanding the landscape of immunotherapy in thymic epithelial tumors.Cancer. 2023 Apr 15;129(8):1162-1172. doi: 10.1002/cncr.34678. Epub 2023 Feb 19. Cancer. 2023. PMID: 36808725 Review.
-
The influence of PD-L1 expression levels on the efficacy of combination therapy in thymic epithelial tumors.Clin Transl Oncol. 2025 Feb;27(2):542-548. doi: 10.1007/s12094-024-03618-x. Epub 2024 Jul 24. Clin Transl Oncol. 2025. PMID: 39046681
Cited by
-
Stem-Cell-Regenerative and Protective Effects of Squid (Symplectoteuthis oualaniensis) Skin Collagen Peptides against H2O2-Induced Fibroblast Injury.Mar Drugs. 2024 May 30;22(6):255. doi: 10.3390/md22060255. Mar Drugs. 2024. PMID: 38921566 Free PMC article.
-
Co-Delivery of aPD-L1 and CD73 Inhibitor Using Calcium Phosphate Nanoparticles for Enhanced Melanoma Immunotherapy with Reduced Toxicity.Adv Sci (Weinh). 2025 Feb;12(7):e2410545. doi: 10.1002/advs.202410545. Epub 2024 Dec 24. Adv Sci (Weinh). 2025. PMID: 39716993 Free PMC article.
-
Spatial Distribution Patterns of Pleural Dissemination in Patients With Thymoma and Survival Analysis.Can Respir J. 2024 Dec 9;2024:4792750. doi: 10.1155/carj/4792750. eCollection 2024. Can Respir J. 2024. PMID: 39687409 Free PMC article.
-
Machine learning for predicting the prognosis of patients with thymoma and thymic carcinoma.J Thorac Dis. 2025 Feb 28;17(2):824-835. doi: 10.21037/jtd-24-1263. Epub 2025 Feb 20. J Thorac Dis. 2025. PMID: 40083535 Free PMC article.
-
Multi-sequence MRI based radiomics nomogram for prediction expression of programmed death ligand 1 in thymic epithelial tumor.Front Immunol. 2025 Apr 11;16:1555530. doi: 10.3389/fimmu.2025.1555530. eCollection 2025. Front Immunol. 2025. PMID: 40292290 Free PMC article.
References
-
- Marx A, Chan JKC, Chalabreysse L, Dacic S, Detterbeck F, French CA, Hornick JL, Inagaki H, Jain D, Lazar AJ, et al. The 2021 WHO classification of tumors of the thymus and mediastinum: what is new in thymic epithelial, germ cell, and mesenchymal tumors? J Thorac Oncol. 2022;17:200–213. doi: 10.1016/j.jtho.2021.10.010. - DOI - PubMed
-
- Berardi R, De Lisa M, Pagliaretta S, Onofri A, Morgese F, Savini A, Ballatore Z, Caramanti M, Santoni M, Mazzanti P, Cascinu S. Thymic neoplasms: an update on the use of chemotherapy and new targeted therapies. A literature review Cancer Treat Rev. 2014;40:495–506. doi: 10.1016/j.ctrv.2013.11.003. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
