

Evaluation of safety and efficacy of autologous oral mucosa-derived epithelial cell sheet transplantation for prevention of anastomotic restenosis in congenital esophageal atresia and congenital esophageal stenosis
- PMID: 37055850
- PMCID: PMC10099682
- DOI: 10.1186/s13287-023-03321-8
Evaluation of safety and efficacy of autologous oral mucosa-derived epithelial cell sheet transplantation for prevention of anastomotic restenosis in congenital esophageal atresia and congenital esophageal stenosis
Abstract
Background: We performed the first autologous oral mucosa-derived epithelial cell sheet transplantation therapy in a patient with refractory postoperative anastomotic stricture in congenital esophageal atresia (CEA) and confirmed its safety. In this study, patients with CEA and congenital esophageal stenosis were newly added as subjects to further evaluate the safety and efficacy of cell sheet transplantation therapy.
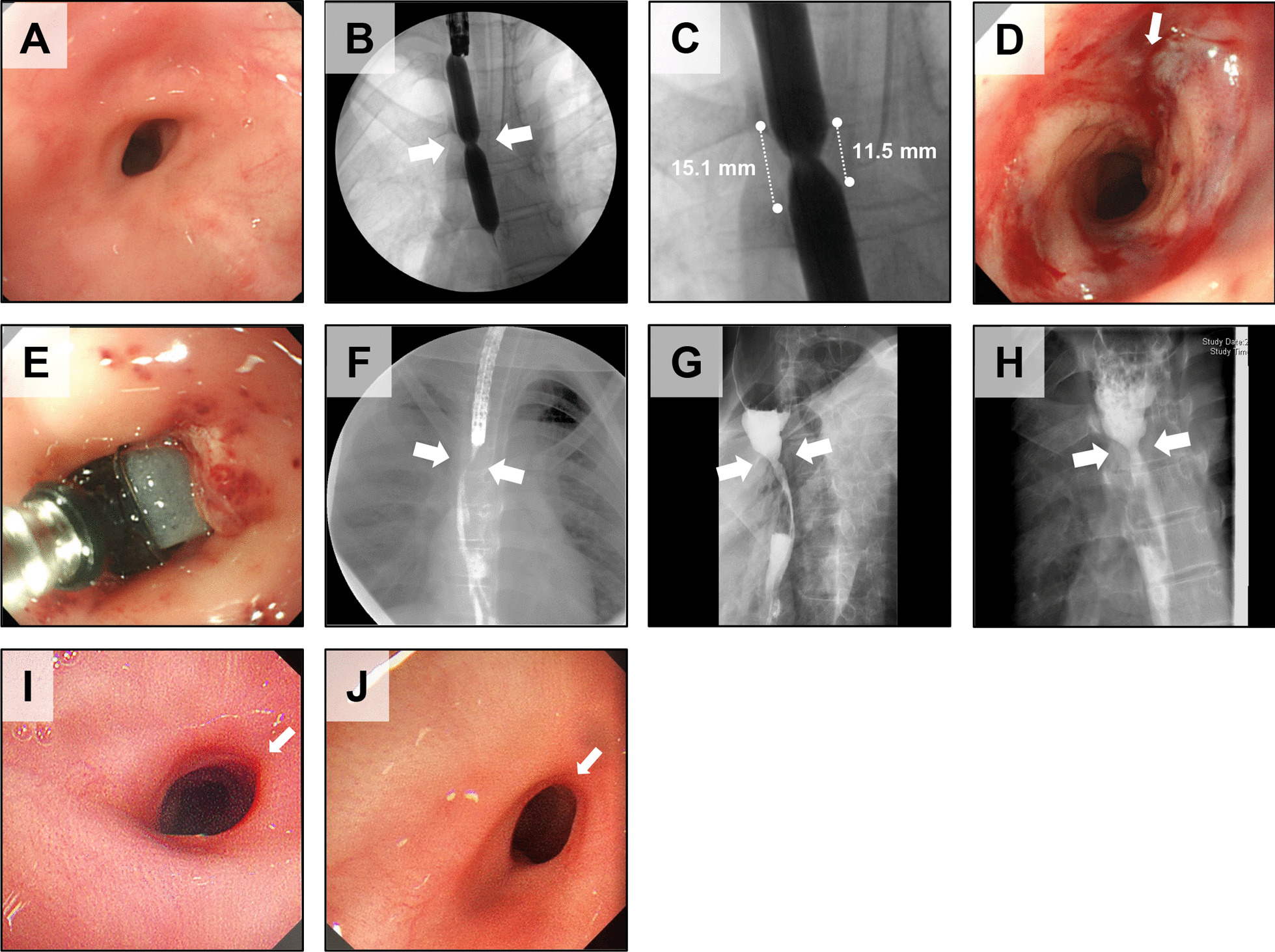
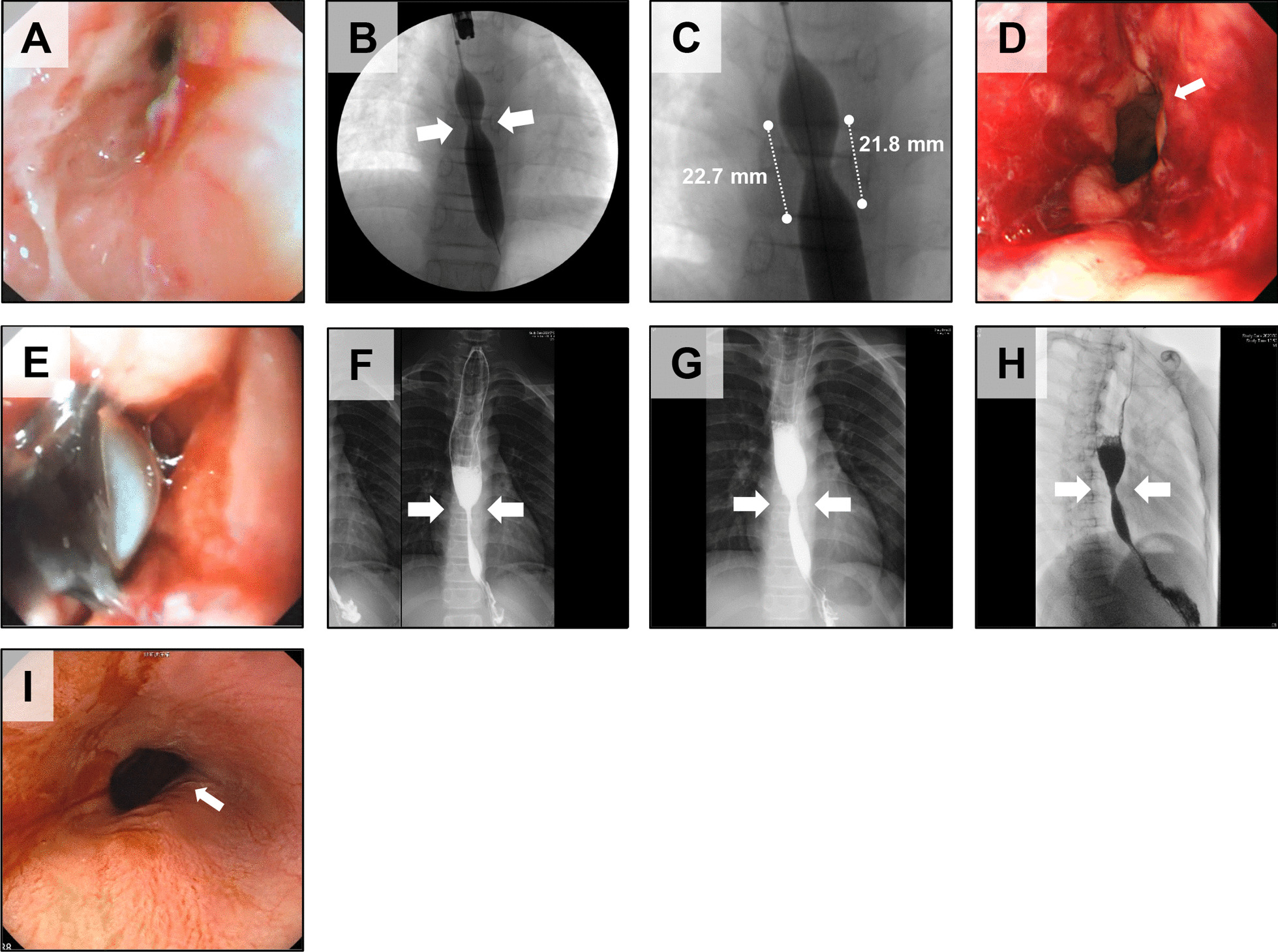
Methods: Epithelial cell sheets were prepared from the oral mucosa of the subjects and transplanted into esophageal tears created by endoscopic balloon dilatation (EBD). The safety of the cell sheets was confirmed by quality control testing, and the safety of the transplantation treatment was confirmed by 48-week follow-up examinations.
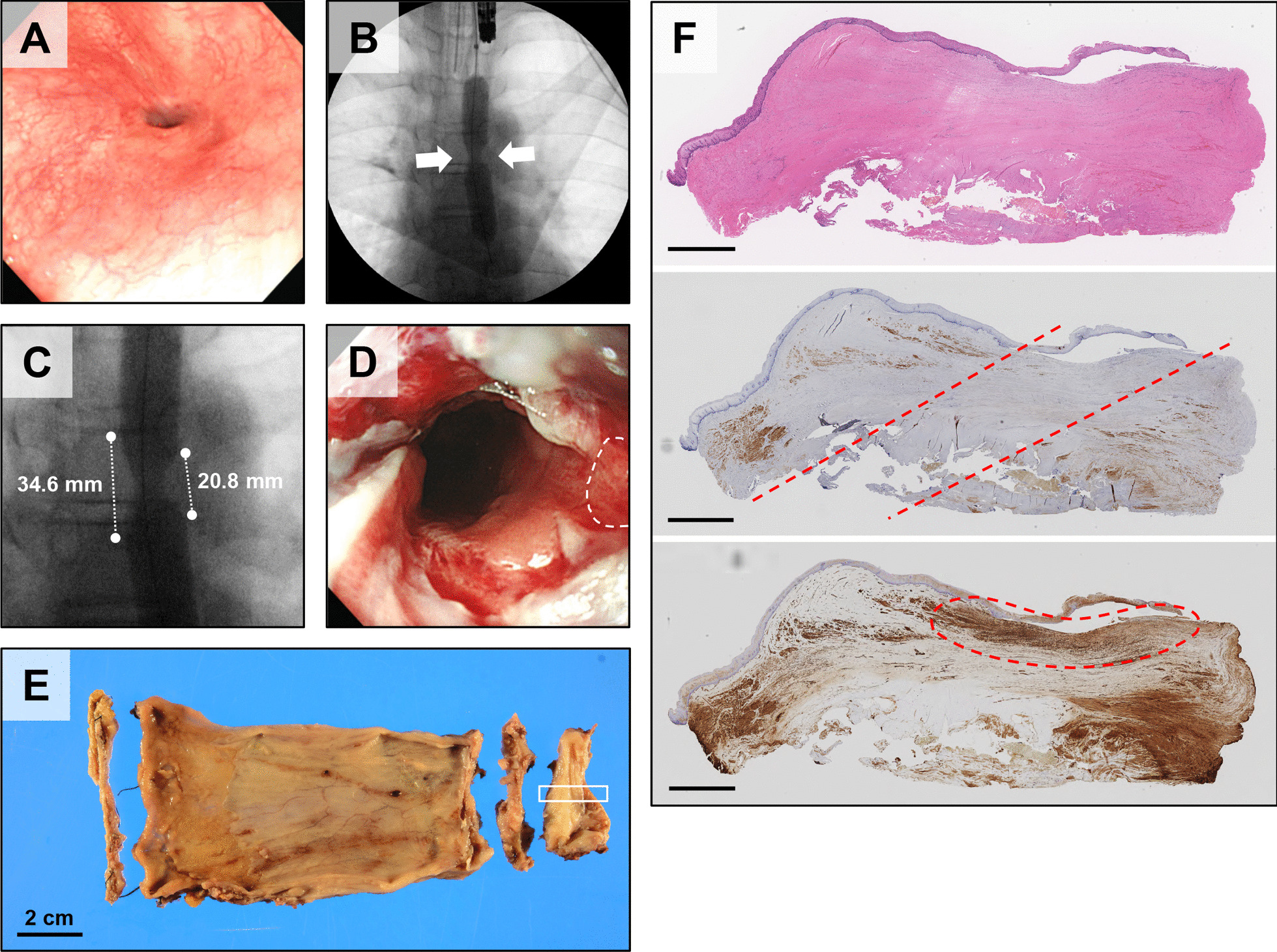
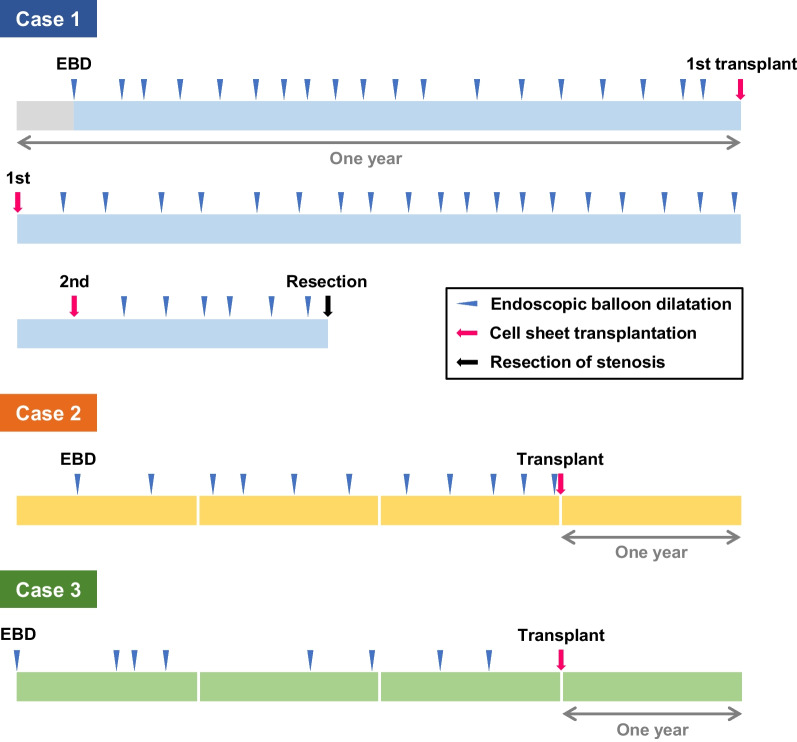
Results: Subject 1 had a stenosis resected because the frequency of EBD did not decrease after the second transplantation. Histopathological examination of the resected stenosis revealed marked thickening of the submucosal layer. Subjects 2 and 3 did not require EBD for 48 weeks after transplantation, during which time they were able to maintain a normal diet by mouth.
Conclusions: Subjects 2 and 3 were free of EBD for a long period of time after transplantation, confirming that cell sheet transplantation therapy is clearly effective in some cases. In the future, it is necessary to study more cases; develop new technologies such as an objective index to evaluate the efficacy of cell sheet transplantation therapy and a device to achieve more accurate transplantation; identify cases in which the current therapy is effective; and find the optimal timing of transplantation; and clarify the mechanism by which the current therapy improves stenosis.
Trial registration: UMIN, UMIN000034566, registered 19 October 2018, https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000039393 .
Keywords: Anastomotic stenosis; Cell sheet transplantation; Congenital esophageal atresia; Congenital esophageal stenosis; Endoscopy; Epithelial cell sheet; Regenerative therapy; Somatic stem cells.
© 2023. The Author(s).
Conflict of interest statement
AU is a co-researcher with CellSeed Inc. MM is the CEO of MakeWay LLC. The other authors have no conflicts of interest regarding the work described herein. AU is the associate editor of the journal and was not involved in the peer review process of the article.
Figures
Similar articles
-
First-in-human autologous oral mucosal epithelial sheet transplantation to prevent anastomotic re-stenosis in congenital esophageal atresia.Stem Cell Res Ther. 2022 Jan 28;13(1):35. doi: 10.1186/s13287-022-02710-9. Stem Cell Res Ther. 2022. PMID: 35090534 Free PMC article.
-
Prevention of esophageal stricture after endoscopic submucosal dissection using tissue-engineered cell sheets.Gastroenterology. 2012 Sep;143(3):582-588.e2. doi: 10.1053/j.gastro.2012.04.050. Epub 2012 May 3. Gastroenterology. 2012. PMID: 22561054
-
Oral epithelial cell sheets engraftment for esophageal strictures after endoscopic submucosal dissection of squamous cell carcinoma and airplane transportation.Sci Rep. 2017 Dec 12;7(1):17460. doi: 10.1038/s41598-017-17663-w. Sci Rep. 2017. PMID: 29234120 Free PMC article. Clinical Trial.
-
Balloon dilatation for congenital esophageal stenosis associated with esophageal atresia.Pediatr Surg Int. 2024 Mar 22;40(1):89. doi: 10.1007/s00383-024-05652-w. Pediatr Surg Int. 2024. PMID: 38517524 Free PMC article. Review.
-
Regenerative medicine: tissue-engineered cell sheet for the prevention of post-esophageal ESD stricture.Gastrointest Endosc Clin N Am. 2014 Apr;24(2):273-81. doi: 10.1016/j.giec.2013.11.003. Epub 2014 Jan 28. Gastrointest Endosc Clin N Am. 2014. PMID: 24679238 Review.
Cited by
-
Therapeutic Intervention in Pediatric Endoscopy: Management of Postsurgical Complications and Bleeding.Visc Med. 2025 May 24. doi: 10.1159/000545893. Online ahead of print. Visc Med. 2025. PMID: 40612537 Free PMC article. Review.
-
Risk factors and prevention and treatment methods of anastomotic stricture after esophageal atresia repair: a literature review.Pediatr Surg Int. 2025 Mar 24;41(1):99. doi: 10.1007/s00383-025-05996-x. Pediatr Surg Int. 2025. PMID: 40126725 Review.
-
Establishment and characterization of multilayered fibroblast cell sheets from the canine oral mucosa, skin, and tail skin.Open Vet J. 2024 Dec;14(12):3428-3439. doi: 10.5455/OVJ.2024.v14.i12.27. Epub 2024 Dec 31. Open Vet J. 2024. PMID: 39927349 Free PMC article.
-
Global trends and research hotspots in esophageal strictures: A bibliometric study.World J Gastrointest Surg. 2025 Mar 27;17(3):100920. doi: 10.4240/wjgs.v17.i3.100920. World J Gastrointest Surg. 2025. PMID: 40162389 Free PMC article.
References
Publication types
MeSH terms
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
