

Cost-effectiveness analysis of 'test and treat' policy for antiretroviral therapy among heterosexual HIV population in India
- PMID: 37056069
- PMCID: PMC10278921
- DOI: 10.4103/ijmr.IJMR_806_20
Cost-effectiveness analysis of 'test and treat' policy for antiretroviral therapy among heterosexual HIV population in India
Abstract
Background & objectives: The World Health Organisation recommended immediate initiation of antiretroviral therapy (ART) in all adult human immunodeficiency virus (HIV) patients regardless of their CD4 cell count. This study was undertaken to ascertain the cost-effectiveness of implementation of these guidelines in India.
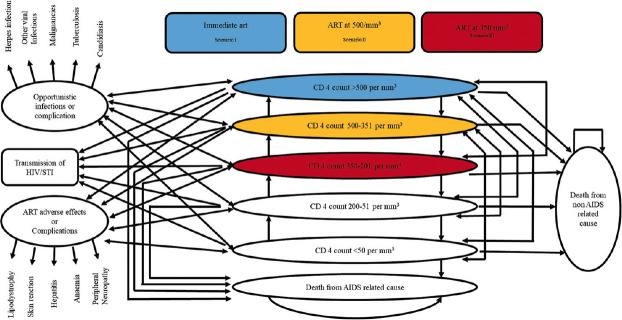
Methods: A Markov model was developed to assess the lifetime costs and health outcomes of three scenarios for initiation of ART treatment at varying CD4 cell count <350/mm[3], <500/mm[3] and test and treat using health system perspective using life-time horizon. A few input parameters for this model namely, transition probabilities from one stage to another stage of HIV and incidence rates of TB were calculated from the data of Centre of Excellence for HIV treatment and care, Chandigarh; whereas, other parameters were obtained from the published literature. Total HIV-related deaths averted, HIV infections averted and incremental cost-effectiveness ratio per quality adjusted life years (QALYs) gained were calculated.
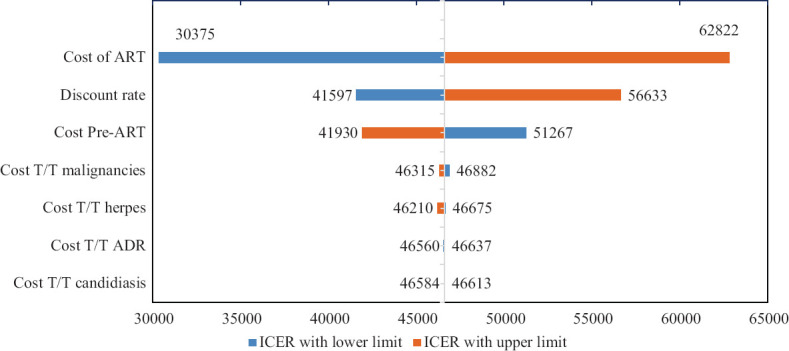
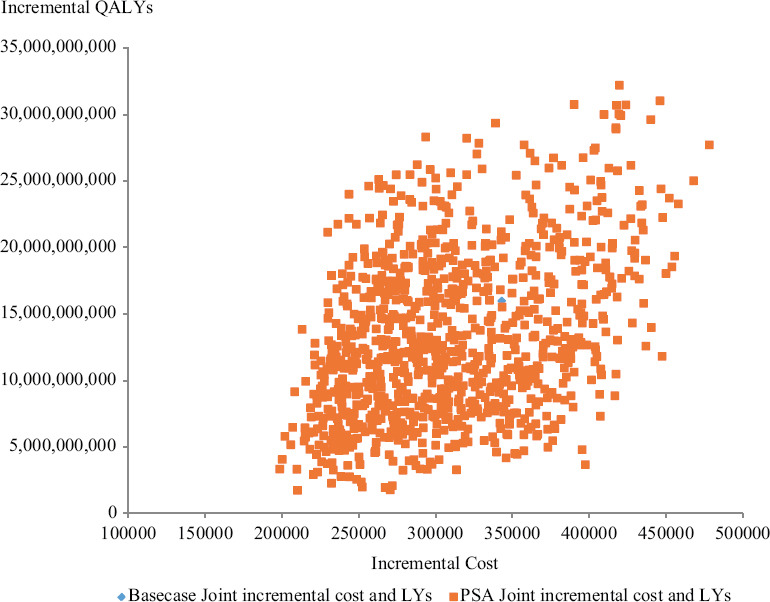
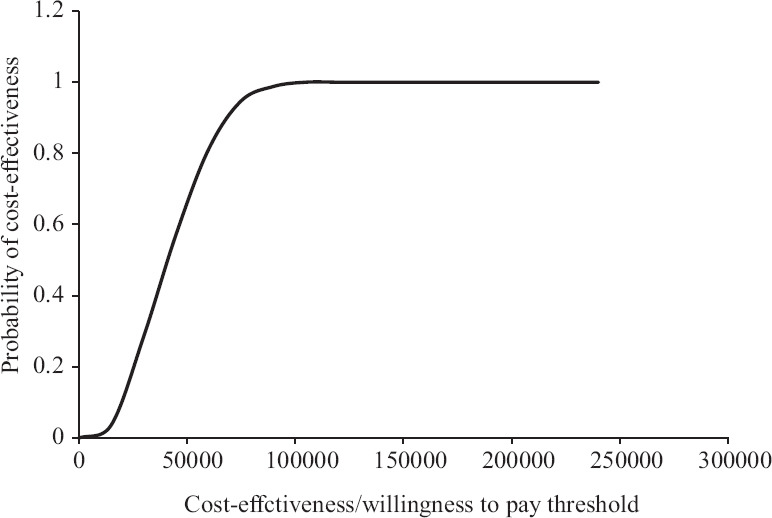
Result: Test and treat intervention slowed down the progression of disease and averted 18,386 HIV-related deaths, over lifetime horizon. It also averted 16,105 new HIV infections and saved 343,172 QALYs as compared to the strategy of starting ART at CD4 cell count of 500/mm[3]. Incremental cost per QALY gained for the immediate initiation of ART as compared to ART at CD4 cell count of 500/mm[3] and 350/mm[3] was ₹ 46,599 and 80,050, respectively at reported rates of adherence to the therapy.
Interpretation & conclusions: Immediate ART (test and treat) is highly cost-effective strategy over the past criteria of delayed therapy in India. Cost-effectiveness of this policy is largely because of reduction in the transmission of HIV.
Keywords: Antiretroviral therapy; CD4; HIV; India –; cost-effectiveness analyses; economic evaluation; modelling; test and treat.
Conflict of interest statement
Figures
Comment on
-
Economic and epidemiological impact of early antiretroviral therapy initiation in India.J Int AIDS Soc. 2015 Oct 1;18(1):20217. doi: 10.7448/IAS.18.1.20217. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26434780 Free PMC article.
References
-
- Sankalak, status of National AIDS Response (Fourth Edition) New Delhi: NACO; 2022. National AIDS Control Organisation. Ministry of Health & Family Welfare, Government of India.
-
- National AIDS Control Organisation. Ministry of Health & Family Welfare, Government of India. Office memorandum. [accessed on November 8, 2021]. Available from: http://naco.gov.in/sites/default/files/Scan_OM%20CST.pdf .
-
- Rewari BB, Agarwal R, Shastri S, Nagaraja SB, Rathore AS. Adoption of the 2015 World Health Organization guidelines on antiretroviral therapy: Programmatic implications for India. WHO South East Asia J Public Health. 2017;6:90–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous