

A Case of Thrombotic Thrombocytopenic Purpura and ST-Elevation Myocardial Infarction: An Unusual Correlation
- PMID: 37056547
- PMCID: PMC10088566
- DOI: 10.7759/cureus.36039
A Case of Thrombotic Thrombocytopenic Purpura and ST-Elevation Myocardial Infarction: An Unusual Correlation
Abstract
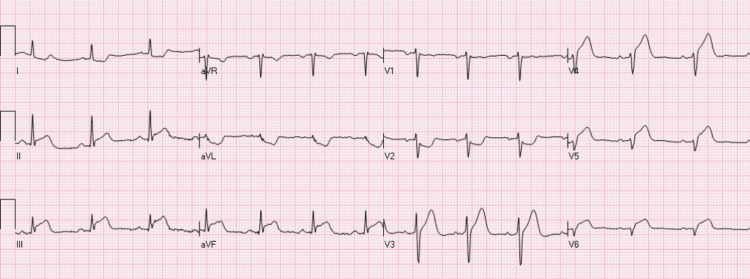
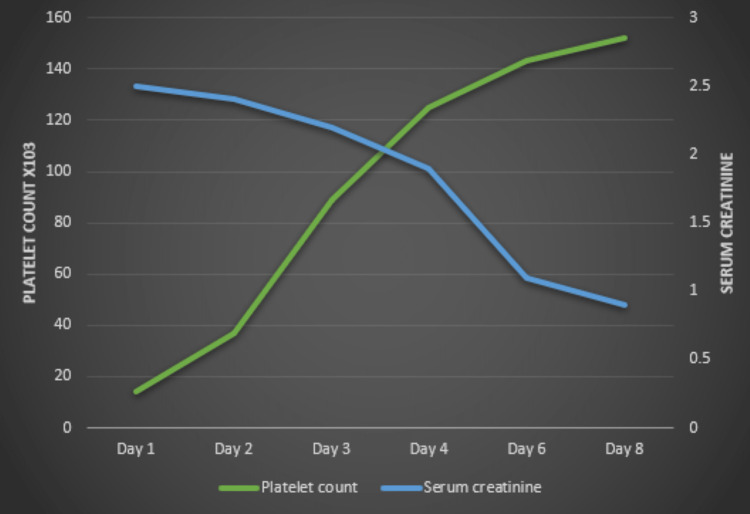
Thrombotic thrombocytopenic purpura (TTP) is a rare and potentially devastating blood disorder depicted by thrombocytopenia, fever, widespread small vessel hemolytic anemia, and neurological symptoms. The involvement of the renal and neurological systems is frequently reported in TTP; however, TTP-induced acute coronary syndrome is not widely reported. We describe a case of myocardial infarction induced by TTP in a patient who presented with the typical manifestation of acute coronary syndrome. Echocardiogram revealed a myocardial injury, and detailed investigations revealed increased levels of troponin I, lactate dehydrogenase, diminished levels of haptoglobin and von Willebrand factor-cleaving protease, and schistocytes on peripheral smear, suggestive of TTP-induced myocardial infarction. His condition was stabilized after commencing plasmapheresis, steroids, and rituximab. The initial steps in the management of this patient involve the prompt administration of steroids and the urgent start of plasmapheresis to increase platelet count.
Keywords: acquired ttp; acute coronary syndrome; acute thrombotic microangiopathy; myocardial infarction; thrombotic thrombocytopenic purpura; ttp.
Copyright © 2023, Omole et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Autoimmune thrombotic microangiopathy: advances in pathogenesis, diagnosis, and management. Tsai HM. Semin Thromb Hemost. 2012;38:469–482. - PubMed
-
- Clinical cardiac involvement in thrombotic thrombocytopenic purpura: a systematic review. Hawkins BM, Abu-Fadel M, Vesely SK, George JN. Transfusion. 2008;48:382–392. - PubMed
-
- Cardiac injury is a common postmortem finding in thrombotic thrombocytopenic purpura patients: is empiric cardiac monitoring and protection needed? Nichols L, Berg A, Rollins-Raval MA, Raval JS. Ther Apher Dial. 2015;19:87–92. - PubMed
-
- Fatal cardiac arrhythmia in a patient with thrombotic thrombocytopenic purpura. Arnold PO, Klink D, Holmes AK. Am J Med Sci. 2006;331:320–321. - PubMed
Publication types
LinkOut - more resources
Full Text Sources