

Performance of point-of-care severity scores to predict prognosis in patients admitted through the emergency department with COVID-19
- PMID: 37057912
- PMCID: PMC11344580
- DOI: 10.1002/jhm.13106
Performance of point-of-care severity scores to predict prognosis in patients admitted through the emergency department with COVID-19
Abstract
Background: Identifying COVID-19 patients at the highest risk of poor outcomes is critical in emergency department (ED) presentation. Sepsis risk stratification scores can be calculated quickly for COVID-19 patients but have not been evaluated in a large cohort.
Objective: To determine whether well-known risk scores can predict poor outcomes among hospitalized COVID-19 patients.
Designs, settings, and participants: A retrospective cohort study of adults presenting with COVID-19 to 156 Hospital Corporation of America (HCA) Healthcare EDs, March 2, 2020, to February 11, 2021.
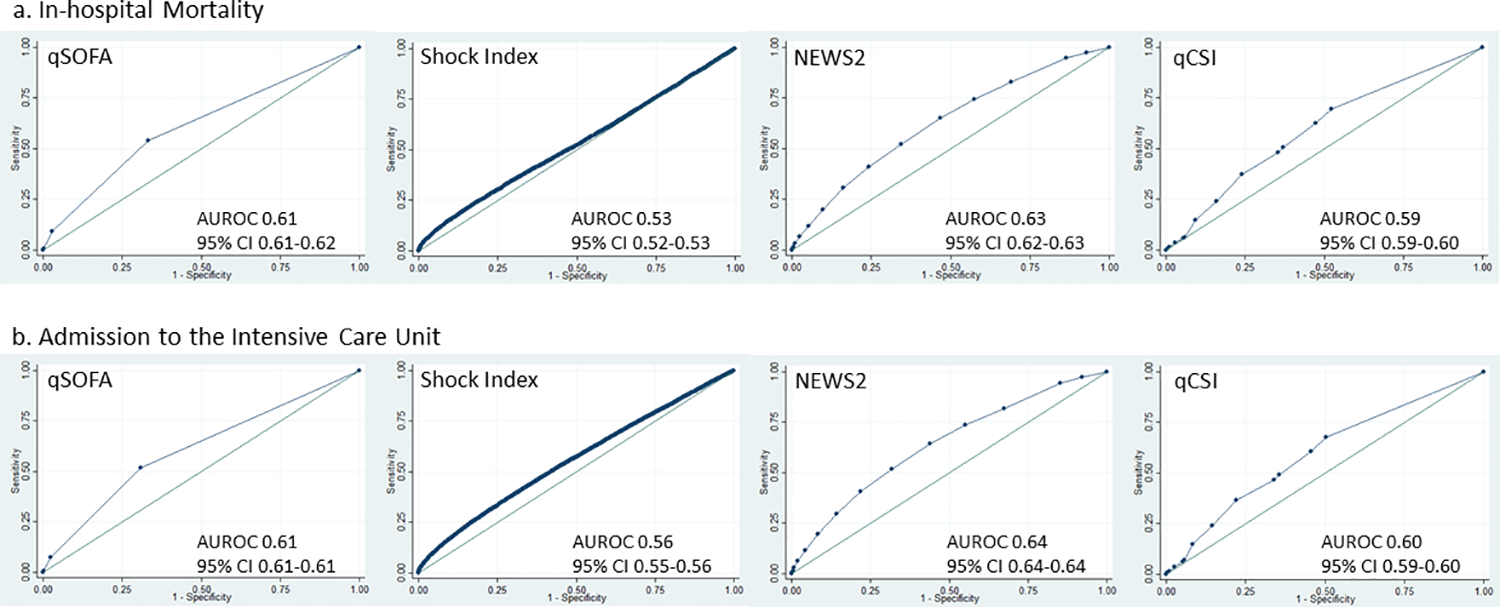
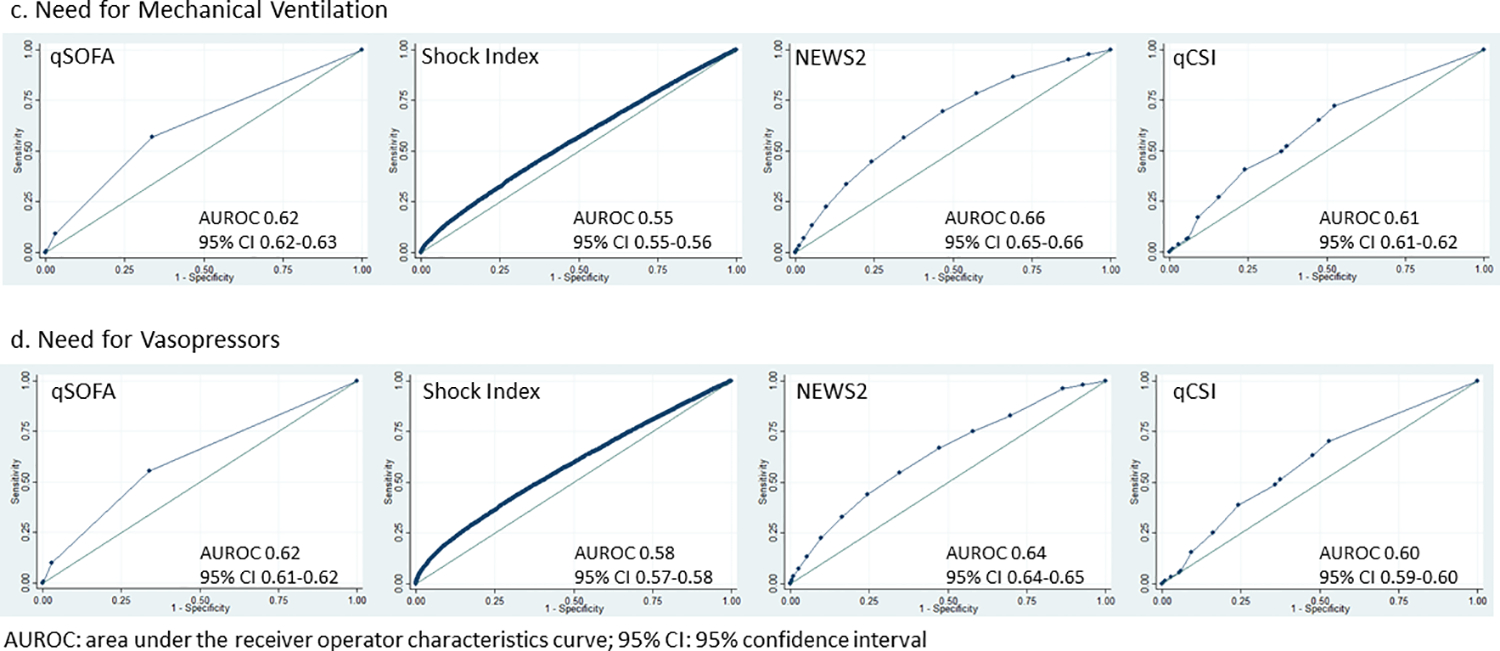
Intervention: Quick Sequential Organ Failure Assessment (qSOFA), Shock Index, National Early Warning System-2 (NEWS2), and quick COVID-19 Severity Index (qCSI) at presentation.
Main outcome and measures: The primary outcome was in-hospital mortality. Secondary outcomes included intensive care unit (ICU) admission, mechanical ventilation, and vasopressors receipt. Patients scored positive with qSOFA ≥ 2, Shock Index > 0.7, NEWS2 ≥ 5, and qCSI ≥ 4. Test characteristics and area under the receiver operating characteristics curves (AUROCs) were calculated.
Results: We identified 90,376 patients with community-acquired COVID-19 (mean age 64.3 years, 46.8% female). 17.2% of patients died in-hospital, 28.6% went to the ICU, 13.7% received mechanical ventilation, and 13.6% received vasopressors. There were 3.8% qSOFA-positive, 45.1% Shock Index-positive, 49.8% NEWS2-positive, and 37.6% qCSI-positive at ED-triage. NEWS2 exhibited the highest AUROC for in-hospital mortality (0.593, confidence interval [CI]: 0.588-0.597), ICU admission (0.602, CI: 0.599-0.606), mechanical ventilation (0.614, CI: 0.610-0.619), and vasopressor receipt (0.600, CI: 0.595-0.604).
Conclusions: Sepsis severity scores at presentation have low discriminative power to predict outcomes in COVID-19 patients and are not reliable for clinical use. Severity scores should be developed using features that accurately predict poor outcomes among COVID-19 patients to develop more effective risk-based triage.
© 2023 Society of Hospital Medicine.
Conflict of interest statement
Dr. Prasad and Ms. Oreper report personal fees from EpiExcellence, LLC outside the submitted work. Dr. Fang’s institution received funding from the National Heart, Lung, and Blood Institute (NHLBI) K24HL141354 and Patient-Centered Outcomes Research Institute. Dr. Auerbach’s institution received funding from the Agency on Healthcare Research and Quality (AHRQ) R01HS027369 and the Moore Foundation Grant 8856. He is also a founder of ADVICE Health, which has no relationship to this work.
Figures
Similar articles
-
Identifying the Sickest During Triage: Using Point-of-Care Severity Scores to Predict Prognosis in Emergency Department Patients With Suspected Sepsis.J Hosp Med. 2021 Aug;16(8):453-461. doi: 10.12788/jhm.3642. J Hosp Med. 2021. PMID: 34328843 Free PMC article.
-
Sepsis patients in the emergency department: stratification using the Clinical Impression Score, Predisposition, Infection, Response and Organ dysfunction score or quick Sequential Organ Failure Assessment score?Eur J Emerg Med. 2018 Oct;25(5):328-334. doi: 10.1097/MEJ.0000000000000460. Eur J Emerg Med. 2018. PMID: 28338533 Free PMC article.
-
Sepsis Clinical Criteria in Emergency Department Patients Admitted to an Intensive Care Unit: An External Validation Study of Quick Sequential Organ Failure Assessment.J Emerg Med. 2017 May;52(5):622-631. doi: 10.1016/j.jemermed.2016.10.012. Epub 2016 Nov 4. J Emerg Med. 2017. PMID: 27823893
-
Comparison of qSOFA and Hospital Early Warning Scores for prognosis in suspected sepsis in emergency department patients: a systematic review.Emerg Med J. 2022 Apr;39(4):284-294. doi: 10.1136/emermed-2020-210416. Epub 2021 Aug 17. Emerg Med J. 2022. PMID: 34404680
-
Evidence reviews for stratifying risk of severe illness or death from sepsis: Suspected sepsis: recognition, diagnosis and early management: Evidence review A.London: National Institute for Health and Care Excellence (NICE); 2024 Jan. London: National Institute for Health and Care Excellence (NICE); 2024 Jan. PMID: 38588370 Free Books & Documents. Review.
Cited by
-
ANCOC Score to Predict Mortality in Different SARS-CoV-2 Variants and Vaccination Status.J Clin Med. 2023 Sep 8;12(18):5838. doi: 10.3390/jcm12185838. J Clin Med. 2023. PMID: 37762779 Free PMC article.
References
-
- COVID Live - Coronavirus Statistics - Worldometer. Accessed August 2, 2022. https://www.worldometers.info/coronavirus/
-
- CDC. Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention. Published February 11, 2020. Accessed August 2, 2022. https://www.cdc.gov/coronavirus/2019-ncov/global-covid-19/rtt-management...
