

DNA-Methylome-Based Tumor Hypoxia Classifier Identifies HPV-Negative Head and Neck Cancer Patients at Risk for Locoregional Recurrence after Primary Radiochemotherapy
- PMID: 37058257
- PMCID: PMC10425733
- DOI: 10.1158/1078-0432.CCR-22-3790
DNA-Methylome-Based Tumor Hypoxia Classifier Identifies HPV-Negative Head and Neck Cancer Patients at Risk for Locoregional Recurrence after Primary Radiochemotherapy
Abstract
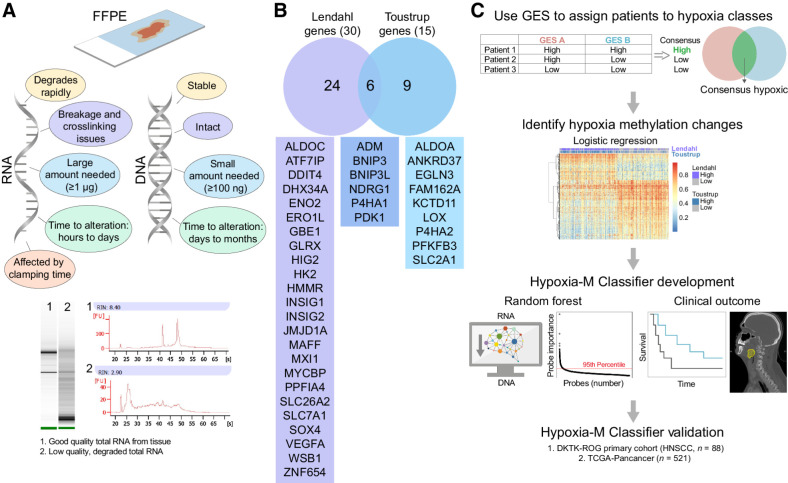
Purpose: Tumor hypoxia is a paradigmatic negative prognosticator of treatment resistance in head and neck squamous cell carcinoma (HNSCC). The lack of robust and reliable hypoxia classifiers limits the adaptation of stratified therapies. We hypothesized that the tumor DNA methylation landscape might indicate epigenetic reprogramming induced by chronic intratumoral hypoxia.
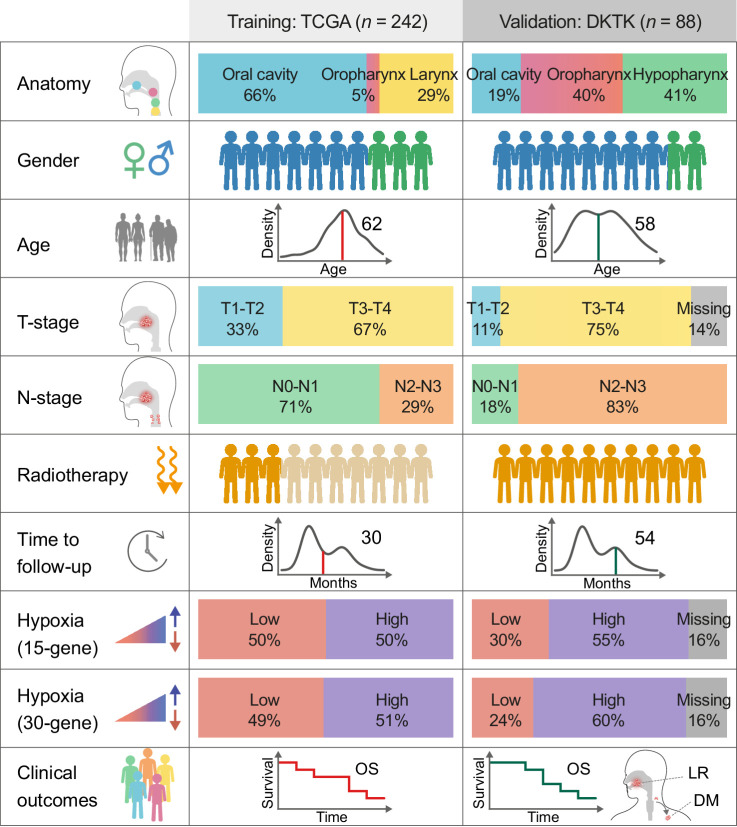
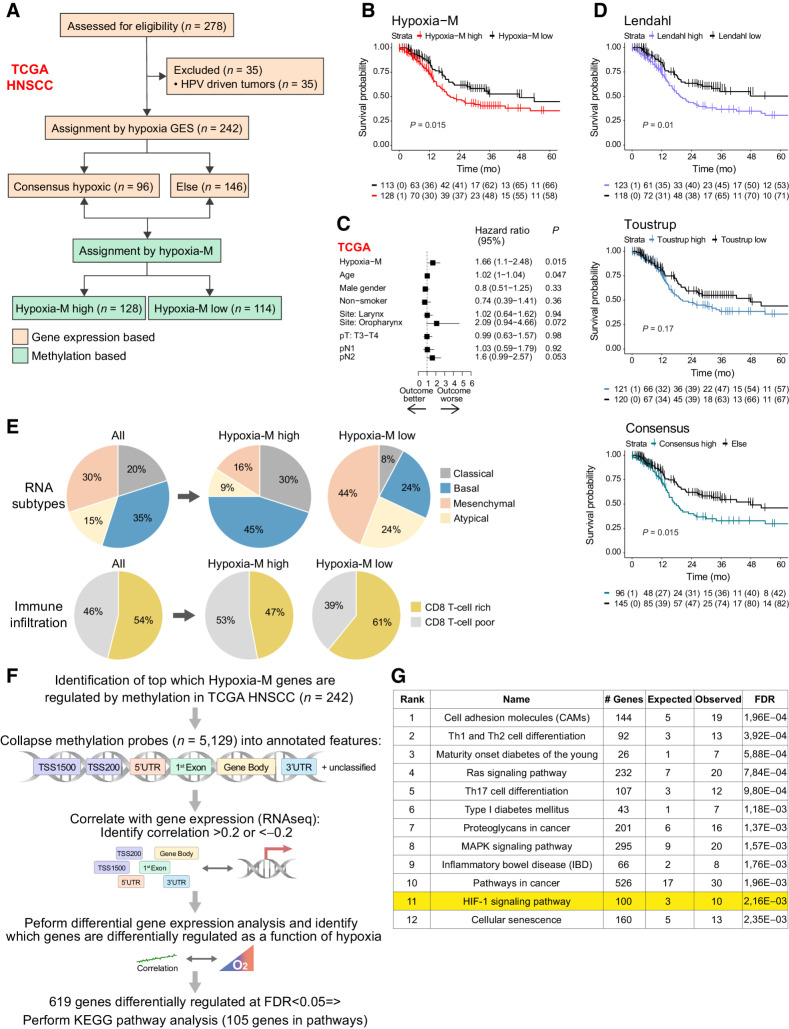
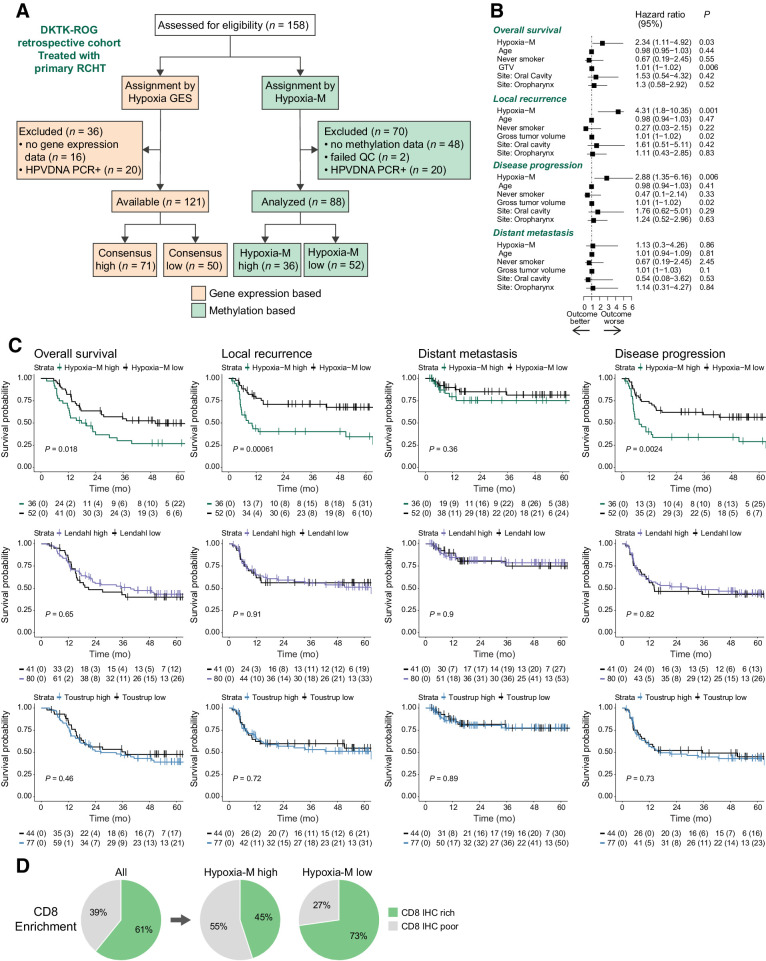
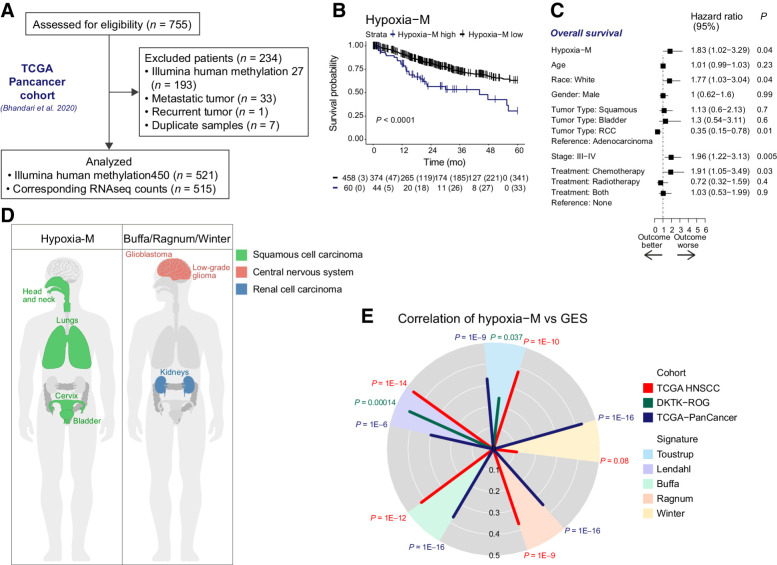
Experimental design: A DNA-methylome-based tumor hypoxia classifier (Hypoxia-M) was trained in the TCGA (The Cancer Genome Atlas)-HNSCC cohort based on matched assignments using gene expression-based signatures of hypoxia (Hypoxia-GES). Hypoxia-M was validated in a multicenter DKTK-ROG trial consisting of human papillomavirus (HPV)-negative patients with HNSCC treated with primary radiochemotherapy (RCHT).
Results: Although hypoxia-GES failed to stratify patients in the DKTK-ROG, Hypoxia-M was independently prognostic for local recurrence (HR, 4.3; P = 0.001) and overall survival (HR, 2.34; P = 0.03) but not distant metastasis after RCHT in both cohorts. Hypoxia-M status was inversely associated with CD8 T-cell infiltration in both cohorts. Hypoxia-M was further prognostic in the TCGA-PanCancer cohort (HR, 1.83; P = 0.04), underscoring the breadth of this classifier for predicting tumor hypoxia status.
Conclusions: Our findings highlight an unexplored avenue for DNA methylation-based classifiers as biomarkers of tumoral hypoxia for identifying high-risk features in patients with HNSCC tumors. See related commentary by Heft Neal and Brenner, p. 2954.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Prognosis to Radiation Unlocked: How Hypoxia Methylome May Hold the Key in HNSCC.Clin Cancer Res. 2023 Aug 15;29(16):2954-2956. doi: 10.1158/1078-0432.CCR-23-1132. Clin Cancer Res. 2023. PMID: 37310809 Free PMC article.
Comment on
-
Prognosis to Radiation Unlocked: How Hypoxia Methylome May Hold the Key in HNSCC.Clin Cancer Res. 2023 Aug 15;29(16):2954-2956. doi: 10.1158/1078-0432.CCR-23-1132. Clin Cancer Res. 2023. PMID: 37310809 Free PMC article.
Similar articles
-
Prognosis to Radiation Unlocked: How Hypoxia Methylome May Hold the Key in HNSCC.Clin Cancer Res. 2023 Aug 15;29(16):2954-2956. doi: 10.1158/1078-0432.CCR-23-1132. Clin Cancer Res. 2023. PMID: 37310809 Free PMC article.
-
Tumor DNA-methylome derived epigenetic fingerprint identifies HPV-negative head and neck patients at risk for locoregional recurrence after postoperative radiochemotherapy.Int J Cancer. 2022 Feb 15;150(4):603-616. doi: 10.1002/ijc.33842. Epub 2021 Nov 8. Int J Cancer. 2022. PMID: 34648658
-
HPV status, cancer stem cell marker expression, hypoxia gene signatures and tumour volume identify good prognosis subgroups in patients with HNSCC after primary radiochemotherapy: A multicentre retrospective study of the German Cancer Consortium Radiation Oncology Group (DKTK-ROG).Radiother Oncol. 2016 Dec;121(3):364-373. doi: 10.1016/j.radonc.2016.11.008. Epub 2016 Nov 29. Radiother Oncol. 2016. PMID: 27913065
-
[Mutation signatures in head and neck squamous cell carcinoma : Pathogenesis and therapeutic potential].HNO. 2020 Dec;68(12):922-926. doi: 10.1007/s00106-020-00954-6. Epub 2020 Oct 12. HNO. 2020. PMID: 33044581 Review. German.
-
Head and neck squamous cell carcinoma: Ambiguous human papillomavirus status, elevated p16, and deleted retinoblastoma 1.Head Neck. 2017 Mar;39(3):E34-E39. doi: 10.1002/hed.24604. Epub 2016 Nov 8. Head Neck. 2017. PMID: 27859938 Free PMC article. Review.
Cited by
-
Epigenetic Targeting to Overcome Radioresistance in Head and Neck Cancer.Cancers (Basel). 2024 Feb 9;16(4):730. doi: 10.3390/cancers16040730. Cancers (Basel). 2024. PMID: 38398123 Free PMC article.
-
Clinical relevance and therapeutic predictive ability of hypoxia biomarkers in head and neck cancer tumour models.Mol Oncol. 2024 Aug;18(8):1885-1903. doi: 10.1002/1878-0261.13620. Epub 2024 Mar 1. Mol Oncol. 2024. PMID: 38426642 Free PMC article.
-
Prognosis to Radiation Unlocked: How Hypoxia Methylome May Hold the Key in HNSCC.Clin Cancer Res. 2023 Aug 15;29(16):2954-2956. doi: 10.1158/1078-0432.CCR-23-1132. Clin Cancer Res. 2023. PMID: 37310809 Free PMC article.
References
-
- Abdollahi A, Folkman J. Evading tumor evasion: current concepts and perspectives of anti-angiogenic cancer therapy. Drug Resist Updat 2010;13:16–28. - PubMed
-
- Salem A, Asselin M-C, Reymen B, Jackson A, Lambin P, West CML, et al. . Targeting hypoxia to improve non–small cell lung cancer outcome. JNCI J Natl Cancer Inst 2018;110:14–30. - PubMed
-
- Toustrup K, Sørensen BS, Metwally MAH, Tramm T, Mortensen LS, Overgaard J, et al. . Validation of a 15-gene hypoxia classifier in head and neck cancer for prospective use in clinical trials. Acta Oncol 2016;55:1091–8. - PubMed
-
- Cutsem EV, Lenz H-J, Furuse J, Tabernero J, Heinemann V, Ioka T, et al. . MAESTRO: a randomized, double-blind phase III study of evofosfamide (Evo) in combination with gemcitabine (Gem) in previously untreated patients (pts) with metastatic or locally advanced unresectable pancreatic ductal adenocarcinoma (PDAC). J Clin Oncol 2016;34:4007.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
